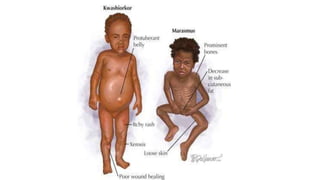
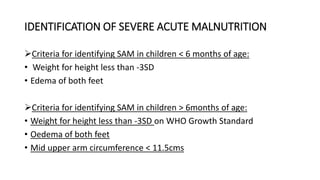
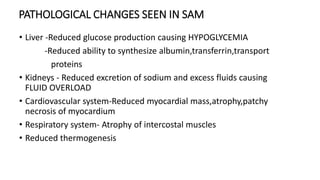
This document discusses severe acute malnutrition (SAM) in children, detailing its definitions, classifications, and clinical syndromes such as marasmus and kwashiorkor. It emphasizes the importance of early detection and treatment criteria, nutritional rehabilitation methods, and prevention strategies, including community health monitoring and specific feeding practices. It underscores the need for comprehensive care that addresses dietary, social, and health factors contributing to malnutrition.