Downloaded 148 times
![The vast majority of children who present acutely with
fever without source (or fever of unclear source) have
underlying infections, typically requiring urgent
evaluation and empirical treatment (especially in young
children). In contrast, fever of unknown origin is not well
defined in children. It has been historically used to
describe a subacute presentation of a single illness of at
least 2 weeks duration during which a fever >38.3°C
(100.9°F) is present for most days and the diagnosis is
unclear after 1 week of intense investigation. [1] The
most common causes are infections,
inflammatory/vasculitic disorders, and malignancies.
These children require a more deliberate, comprehensive,
and prolonged evaluation, and frequently do not need
urgent empirical therapy.](https://image.slidesharecdn.com/feverwithoutasourcepediatrics-151101130453-lva1-app6892/85/Fever-without-a-source-pediatrics-7-320.jpg)
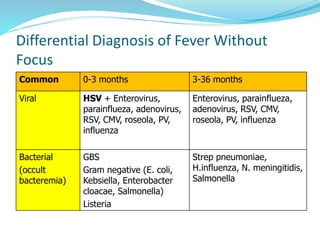
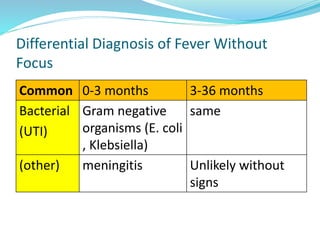
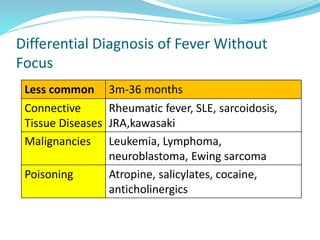
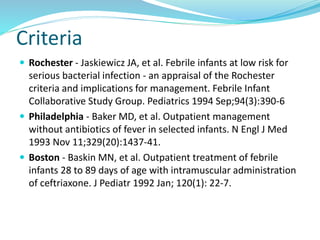
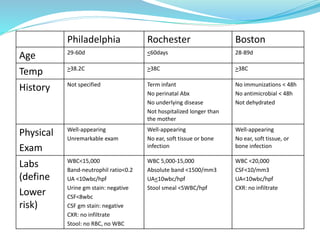
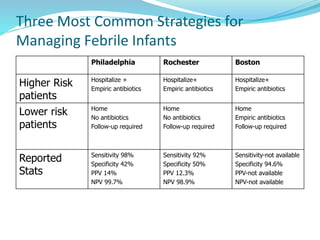

Fever is a common reason for pediatric visits. The hypothalamus regulates body temperature and fever occurs when its set point is elevated. Fever without a source is difficult to diagnose and can be caused by infections, inflammatory disorders, or malignancies. Evaluation involves history, exam, labs including blood cultures, and imaging if indicated. Lower risk children based on criteria like Rochester may be managed as outpatients without antibiotics. Higher risk children receive empiric antibiotics targeting common pathogens until diagnosis is made. Antipyretics and antivirals are also used for symptom relief in some cases.











































































































