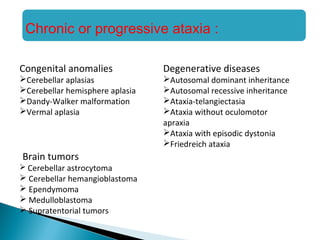
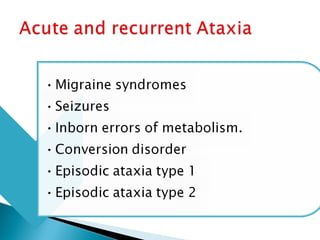
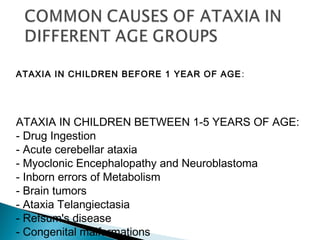
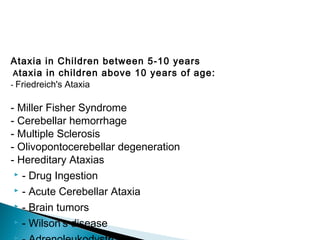
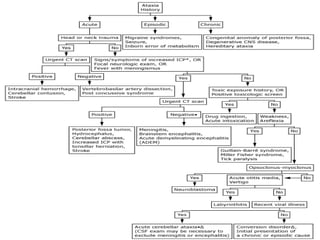
Ataxia is a movement disorder characterized by unsteady gait and is often due to cerebellar dysfunction. It can be acute or chronic and has various causes, including infections, toxins, and congenital conditions, particularly in children. Diagnosis typically requires exclusion of serious illnesses, and while mild cases may resolve spontaneously, more severe situations may require specialized interventions.