1. The document provides an overview of Pediatric Advanced Life Support (PALS) including normal vital signs, basic life support, high quality CPR, the pediatric systematic approach, the pediatric assessment triangle, primary and secondary surveys, post-resuscitation care, pediatric trauma key points, and Covid-19 resuscitation updates.
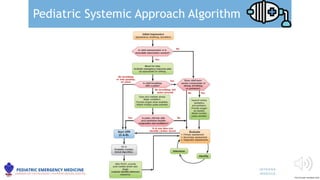
2. It reviews algorithms for the pediatric systematic approach, cardiac arrest, bradycardia, tachycardia, and return of spontaneous circulation.
3. Guidelines are provided for assessment, emergency management, ventilation, circulation, neurologic goals, and personal protective equipment for Covid-19 patients.