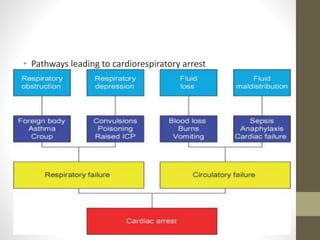
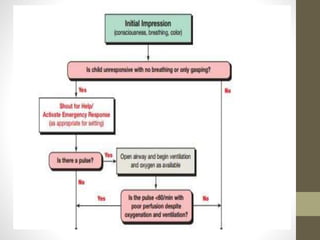
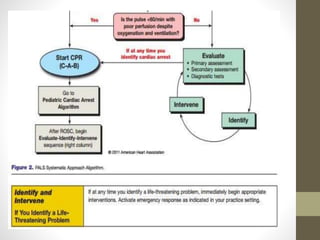
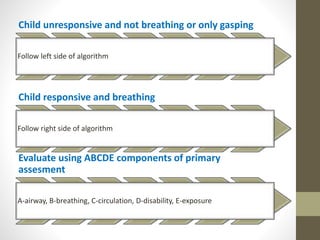
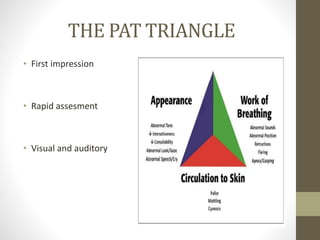
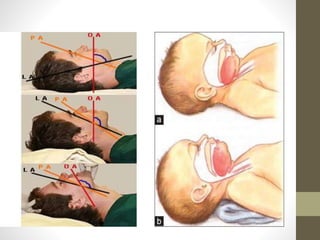
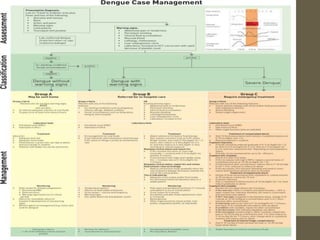
The document provides guidance on assessing and managing pediatric emergencies using the PALS (Pediatric Advanced Life Support) approach. It emphasizes recognizing seriously ill children through a systematic evaluation of the ABCDE (Airway, Breathing, Circulation, Disability, Exposure). Key interventions include proper triage, high-quality CPR, fluid resuscitation, and stabilizing the child. The PALS process involves evaluating, identifying the type and severity of the problem, and then intervening with appropriate treatment such as oxygen, positioning, or medication administration.













































![[CPCR] CARDIOPULMONARY CEREBREAL RESUSCITATION PROCEDURES](https://cdn.slidesharecdn.com/ss_thumbnails/cardiopulmonaryresuscitation-250329164131-a99bc90d-thumbnail.jpg?width=640&height=640&fit=bounds)


























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









