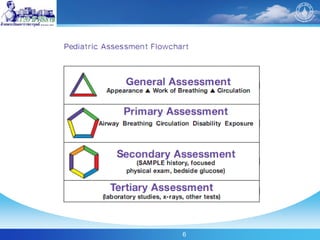
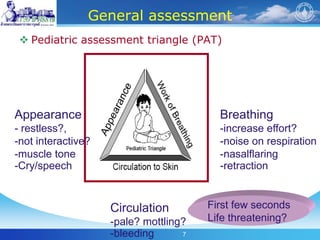
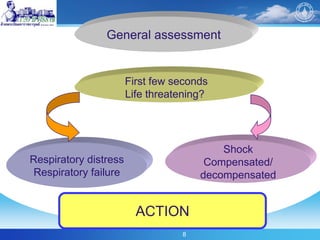
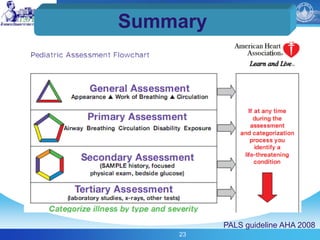
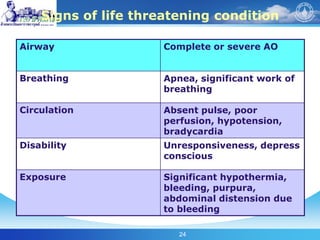
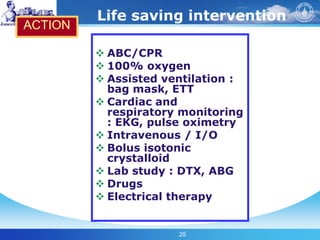
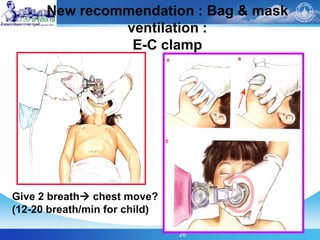
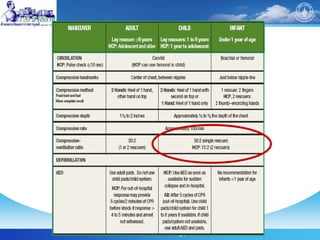
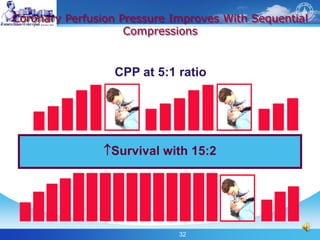
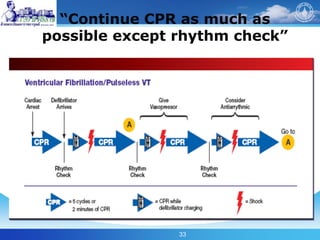
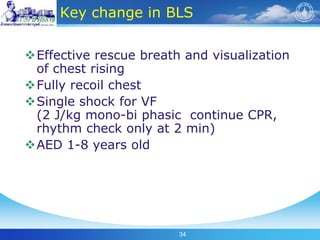
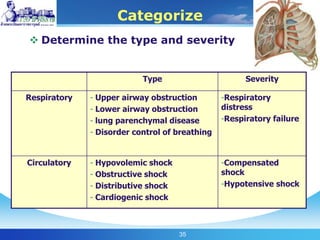
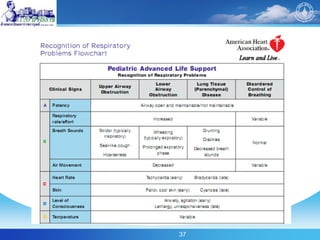
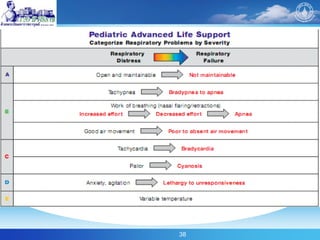
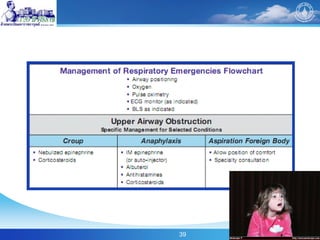
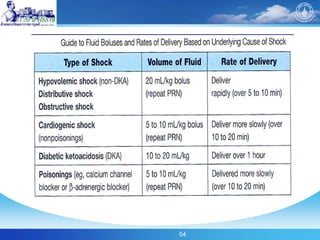
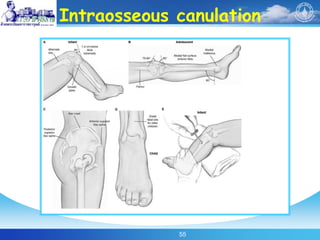
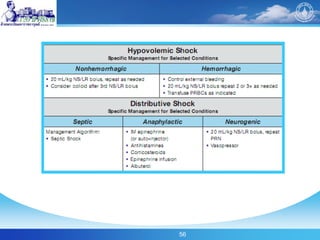
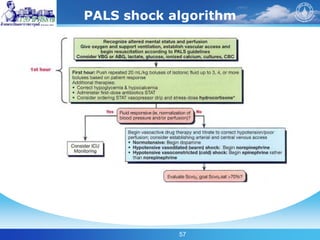
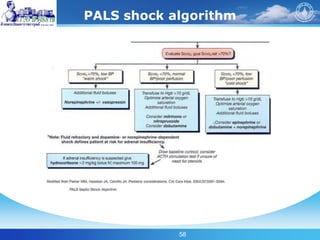
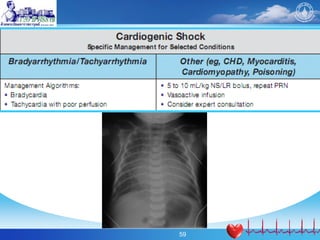
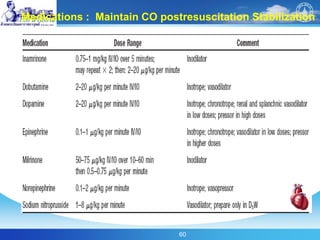
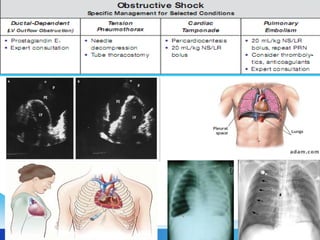
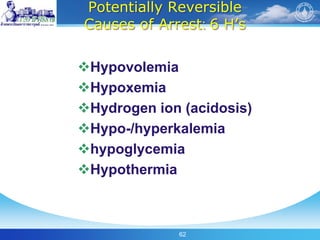
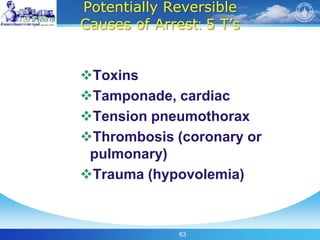
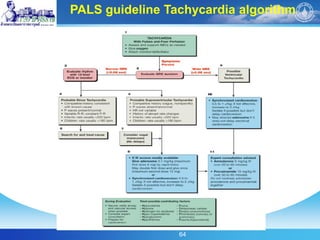
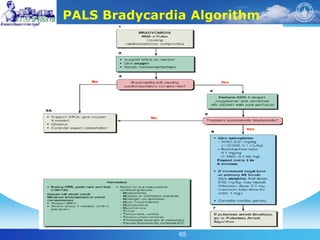
This document summarizes key points from PALS guidelines regarding pre-hospital and emergency care. It discusses conducting a primary assessment of airway, breathing, circulation, disability and exposure. Signs of life-threatening conditions are outlined. The document also summarizes recommendations for chest compressions, endotracheal intubation, use of cuffed tubes, laryngeal masks and verifying tube placement. Recognition of shock in pediatric patients is covered, including etiologies and algorithms for treatment. Potentially reversible causes of cardiac arrest are listed. Trends in PALS, such as the pediatric assessment triangle and cardiocerebral resuscitation, are also mentioned.