

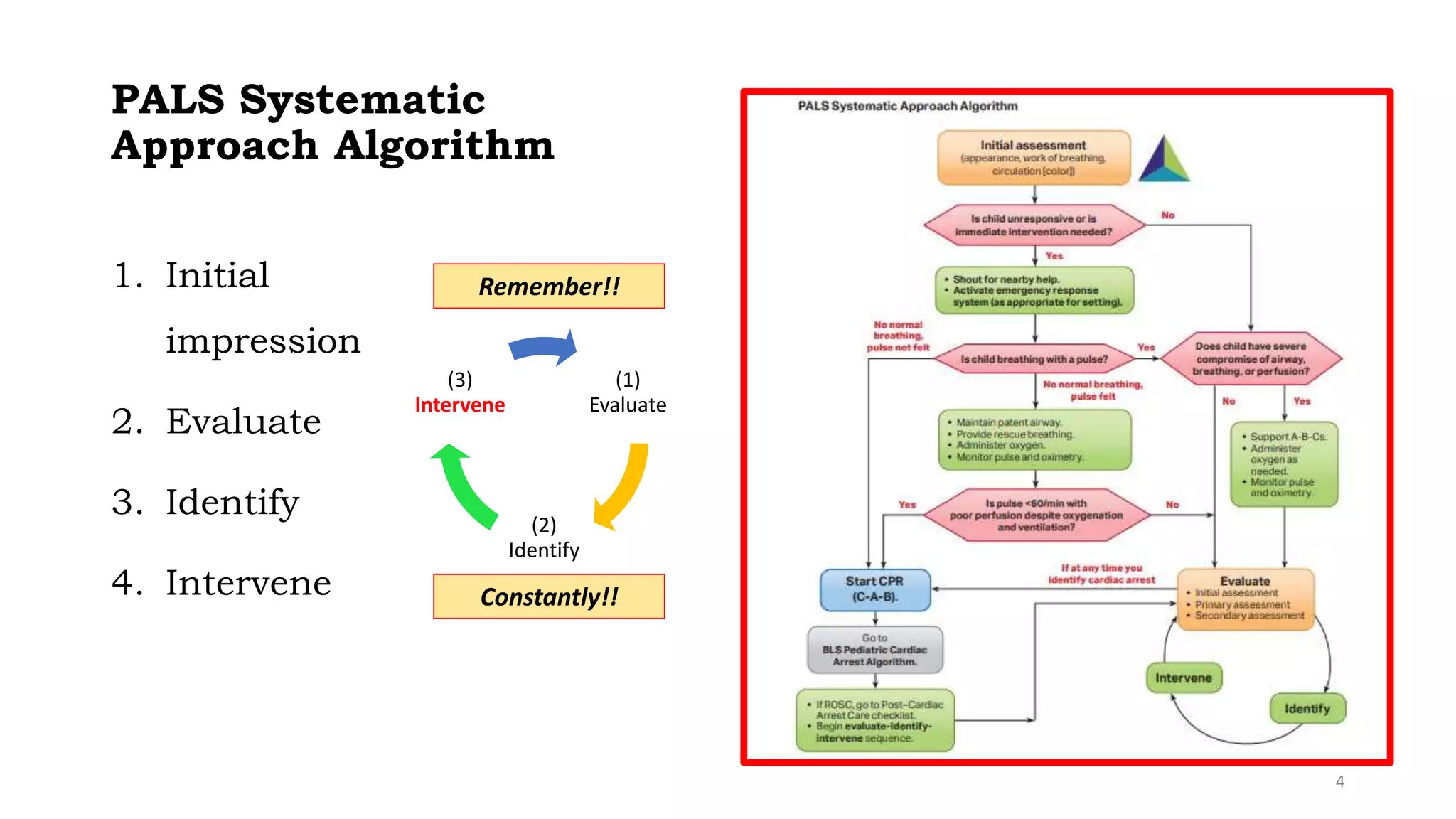



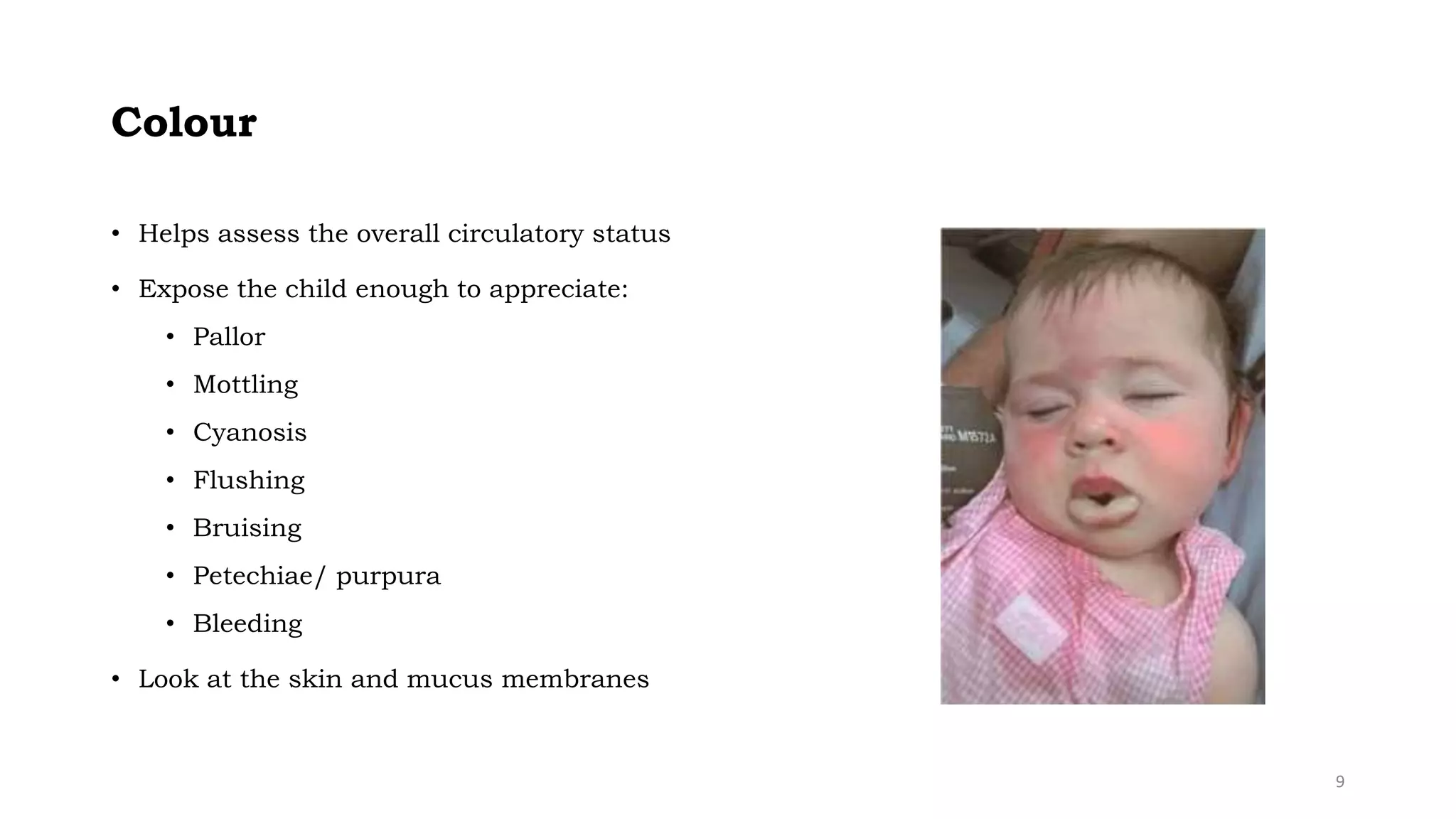



















This document provides an overview of pediatric emergency management for respiratory issues. It outlines a systematic PALS approach of initial impression, evaluation, identification, and intervention. Key points include using the pediatric assessment triangle for initial evaluation, performing a primary ABCDE assessment, identifying the type and severity of respiratory distress or failure, and appropriate oxygen therapy interventions like low-flow nasal cannula or high-flow non-rebreathing mask. The focus is on recognizing respiratory emergencies and applying a structured approach to evaluation and treatment as a team.























































































