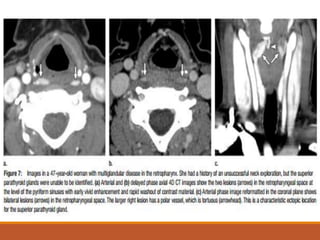
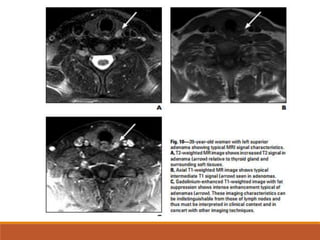
The parathyroid glands are located posterior to the thyroid gland in the neck. Parathyroid adenomas, the most common cause of primary hyperparathyroidism, enhance vividly on arterial phase CT then wash out rapidly on delayed phase with low attenuation on non-contrast images. Localizing the adenoma precisely with 4D CT guides focused surgical treatment through a small incision. The characteristic enhancement pattern and morphology help identify ectopic adenomas located during fetal development in the mediastinum.