Downloaded 2,084 times
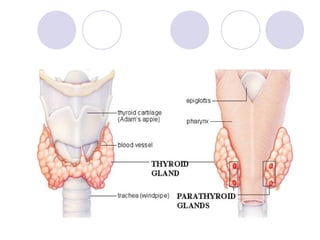
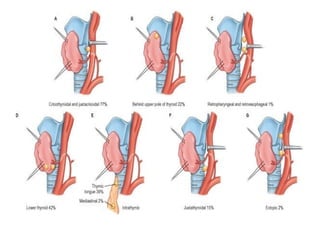
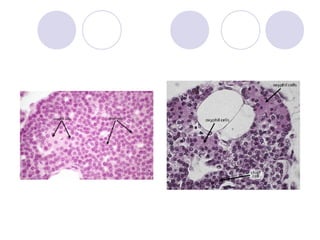
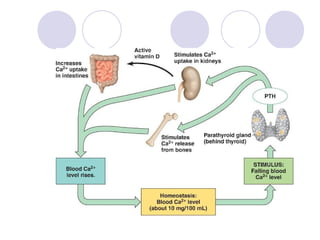
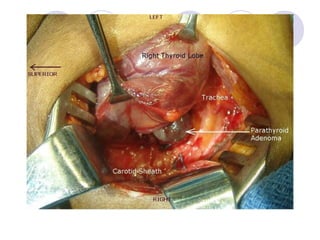

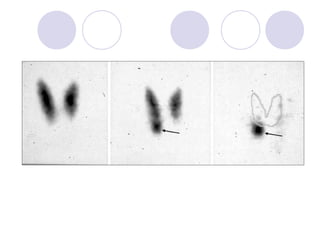




The parathyroid glands are small endocrine glands located on the thyroid gland that secrete parathyroid hormone (PTH) to regulate calcium levels. Primary hyperparathyroidism is usually caused by a solitary parathyroid adenoma. Pre-operative localization with sestamibi scanning is accurate for adenomas. Surgical treatment involves either unilateral or bilateral neck exploration to remove the abnormal gland(s), with minimally invasive radioguided parathyroidectomy being an option for localized disease.



























































![Nasal septum and its diseases[1]](https://cdn.slidesharecdn.com/ss_thumbnails/nasalseptumanditsdiseases1-140421073429-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



















