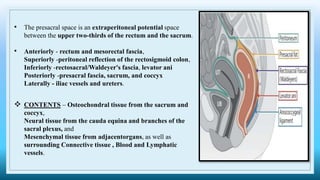
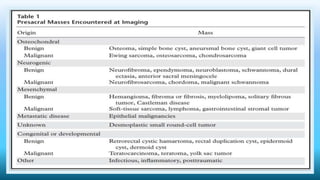
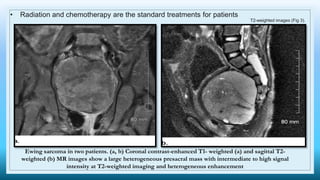
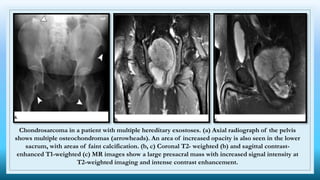
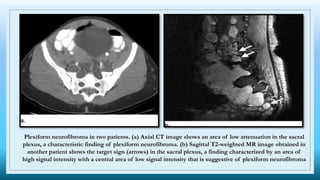
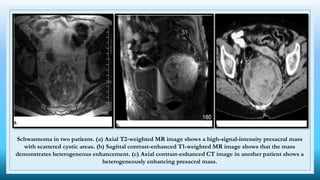
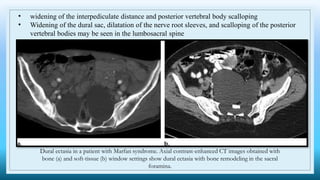
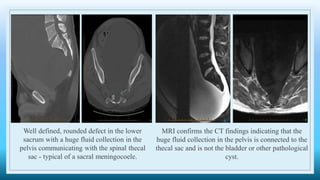
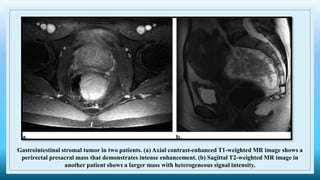
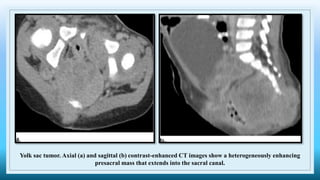
The document discusses various presacral lesions that can be seen on imaging. It describes the anatomy of the presacral space and then covers conditions with osteochondral origin like giant cell tumor and Ewing sarcoma. Neurogenic conditions such as neurofibromas, schwannomas, and perineural cysts are also discussed. Other lesions mentioned include dural ectasia and anterior myelomeningoceles. For each condition, the document provides details on clinical features, imaging appearance on modalities like CT and MRI, and examples of imaging findings.