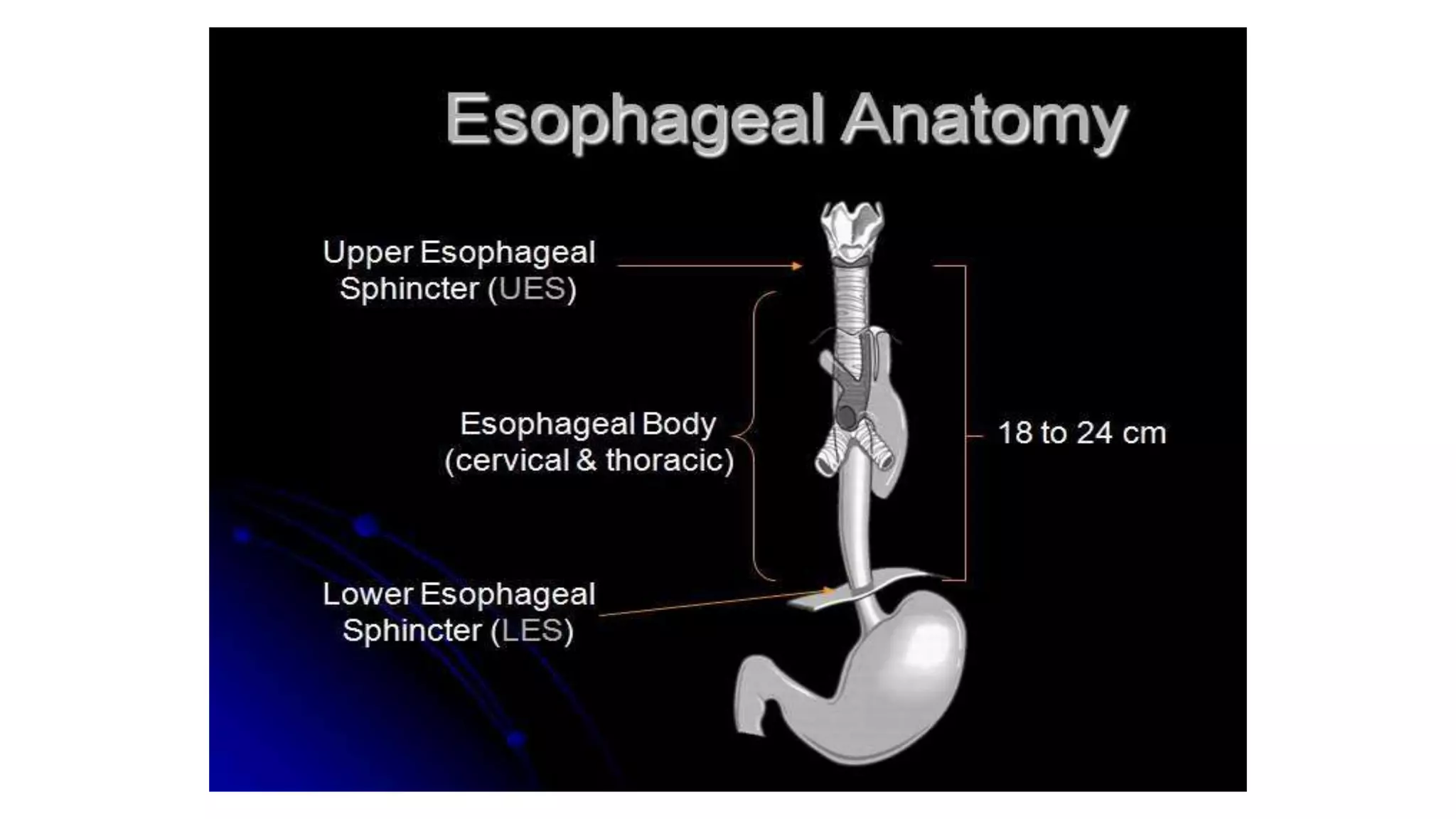
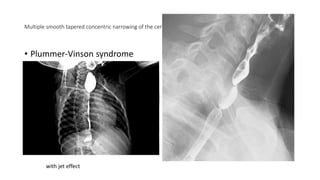
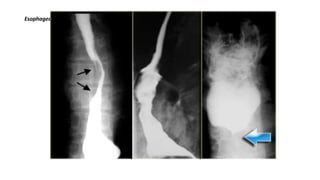
Esophageal webs are thin mucosal membranes that project into the esophageal lumen, causing constriction. They more commonly occur in the cervical esophagus near the cricopharyngeus muscle. Associations include Plummer-Vinson syndrome, graft-versus-host disease, and gastroesophageal reflux disease. On barium swallows, esophageal webs appear as smooth tapered concentric narrowing in the cervical esophagus.



















![OESOPHAGEAL ANATOMY AND PATHOLOGIES (2) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/oesophagealanatomyandpathologies2autosaved-250917094352-40c57836-thumbnail.jpg?width=640&height=640&fit=bounds)




















































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)










