ETIOPATHOGENESIS , CLINICALFEATURES,
INVESTIGATIONS AND SURGICAL
MANAGEMENT OF PRIMARY
HYPERPARATHYROIDISM
BY DR K CHANAKYA SRIVATSA
PGY1 – S1UNIT
UNDER THE GUIDANCE OF DR N SRINIVASARAO SIR
2.
EMBRYOLOGY
• the superiorparathyroid glands are derived from the fourth branchial
pouch
• The third branchial pouches give rise to the inferior para thyroid
glands.
• The position of normal superior parathyroid glands is more consistent,
with 80% of these glands being found near the posterior aspect of the
upper and middle thyroid lobes, at the level of the cricoid cartilage.
3.
ANATOMY
• The superiorglands usually are dorsal to the RLN at the level of the
cricoid cartilage, whereas the inferior parathyroid glands are located
ventral to the nerve.
• Normal parathyroid glands are gray and semitransparent in newborns
but appear golden yellow to light brown in adults.
• Parathyroid glands usually derive their blood supply from branches of
the inferior thyroid artery, although branches from the superior
thyroid artery supply at least 20% of upper glands
• . The parathyroid glands drain ipsilaterally by the superior, middle,
and inferior thyroid veins.
4.
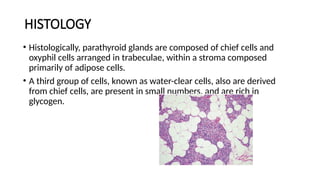
HISTOLOGY
• Histologically, parathyroidglands are composed of chief cells and
oxyphil cells arranged in trabeculae, within a stroma composed
primarily of adipose cells.
• A third group of cells, known as water-clear cells, also are derived
from chief cells, are present in small numbers, and are rich in
glycogen.
5.
PARATHYROID FUNCTIONS
• Thechief function of parathyroid is calcium homeostasis with the help
of the parathormone.
• The parathyroid cells rely on a G-protein–coupled membrane
receptor, designated the calcium sensing receptor (CASR), to regulate
PTH secretion
• PTH secretion also is stimulated by low levels of 1,25-dihydroxy
vitamin D, cat echolamines, and hypomagnesemia..
• . PTH is synthesized in the parathyroid gland as a precursor hormone
preproPTH, which is cleaved first to pro PTH and then to the final 84-
amino-acid PTH.
PRIMARY HYPERPARATHYROIDISM
• PHPToccurs in 0.1% to 0.3% of the general population and is more
common in women (1:500) than in men (1:2000)
• Increased PTH production leads to hypercalcemia via increased GI
absorption of calcium, increased production of vitamin D3 , and
reduced renal calcium clearance
• PHPT is characterized by increased parathyroid cell proliferation and
PTH secretion that is independent of calcium levels.
9.
ETIOLOGY
• The exactcause of PHPT is unknown
• although exposure to low-dose therapeutic ionizing radiation and familial
• Various diets and intermittent exposure to sunshine may also be related.
• renal leak of calcium and declining renal function with age as well as alteration in
the sensitivity of parathyroid glands to suppression by calcium.
• Lithium therapy has been known to shift the set point for PTH secre tion in
parathyroid cells, thereby resulting in elevated PTH lev els and mild
hypercalcemia
• PHPT results from the enlargement of a single gland or parathyroid adenoma in
approximately 80% of cases, multiple adenomas or hyperplasia in 15% to 20% of
patients, and parathyroid carcinoma in 1% of patients
10.
• PHPT alsooccurs within the spectrum of a number of inherited as
MEN1, MEN2A, isolated familial HPT, and familial HPT with jaw-tumor
syndrome
RENAL DISEASE.
• Approximately80% of patients with PHPT have some degree of renal dysfunction
or symptoms.
• The calculi are typically com posed of calcium phosphate or oxalate.
• Nephrocalcinosis, which refers to renal parenchymal calcification, is found in <5%
of patients and is more likely to lead to renal dysfunction.
• Chronic hypercalcemia also can impair concentrating ability, thereby resulting in
polyuria, polydipsia, and nocturia.
• The incidence of hypertension is variable but has been reported to occur in up to
50% of patients with PHPT.
• Hypertension appears to be more common in older patients and correlates with
the magnitude of renal dysfunction
13.
BONE DISEASE.
• Bonedisease, including osteopenia, osteoporosis, and osteitis fibrosa
cystica, is found in about 15% of patients
14.
GASTROINTESTINAL COMPLICATIONS
• PHPThas been associated with peptic ulcer disease. In experimental
animals, hypergastrinemia has been shown to result from PTH
infusion into blood vessels supplying the stomach, independent of its
effects on serum calcium.
• An increased incidence of pancreatitis also has been reported in
patients with PHPT, although this appears to occur only in patients
with profound hypercalcemia (Ca2+ ≥12.5 mg/dL).
• Patients with PHPT also have an increased incidence of cholelithiasis,
presumably due to an increase in biliary calcium, which leads to the
formation of calcium bilirubinate stones.
15.
NEUROPSYCHIATRIC COMPLICATIONS.
• floridpsychosis, depression, or coma
• Studies demonstrate that levels of certain neurotransmitters
(monoamine metabolites 5-hydroxyindoleacetic acid and homovanillic
acid) are reduced in the cerebrospinal fluid of patients with PHPT
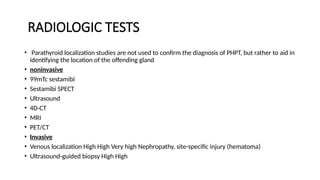
RADIOLOGIC TESTS
• Parathyroidlocalization studies are not used to confirm the diagnosis of PHPT, but rather to aid in
identifying the location of the offending gland
• noninvasive
• 99mTc sestamibi
• Sestamibi SPECT
• Ultrasound
• 4D-CT
• MRI
• PET/CT
• Invasive
• Venous localization High High Very high Nephropathy, site-specific injury (hematoma)
• Ultrasound-guided biopsy High High
18.
TREATMENT
• Medical optionsfor treating PHPT and its complications include
antiresorptive treatments such as bisphosphonates, hor mone
replacement therapy (HRT), and selective estrogen recep tor
modulators such as raloxifene.
19.
SURGICAL TREATMENT
• Indicationsof parathyroidectomy
• Symptomatic patients(patients who have developed complications and have “classic” symptoms of PHPT should
undergo parathyroidectomy)
• Indications of parathyroidectomy in asymptomatic patients
• Age <50 years
• Serum calcium concentration >1 mg/dL (>0.25 mM/liter) above upper limit of normal
• Bone density:
• T-score ≤2.5 at lumbar spine, femoral neck, total hip, or distal one third radius (perimenopausal or
postmenopausal women and men ≥50 years old)
• Z-score ≤2.5 at lumbar spine, femoral neck, total hip, or distal one third radius (premenopausal women and men
<50 years old)
• Vertebral fracture (including fragility fracture) present on radiologic evaluation
• Renal function:
• Creatinine clearance <60 mL/min
• Radiologic evidence of renal stones or nephrocalcinosis (x-ray, ultrasound,computed tomography)
20.
PREOPERATIVE LOCALIZATION TESTS.
•1) Sestamibi-technetium 99m scan
• pros - Allows planar and SPECT imaging
• Cons - False-positive tests due to thyroid neoplasms, lymphadenopathy
• 2) Ultrasound
• Pros- Identification of juxta- and intrathyroidal tumors, Relatively
inexpensive
• cons- False-positive results due to thyroid nodules, cysts, lymph nodes,
esophageal lesions
-False-negatives result from substernal, ectopic, and undescended tumors
21.
• CT scan
•Pros - Localization of ectopic (mediastinal) glands Not useful for juxta-
or intrathyroidal glands
• cons - False-positive results from lymph nodes
- Relatively high cost
- Radiation exposure
22.
• MRI scan
•pros-
-Localization of ectopic tumors
-No radiation exposure
• Cons - False-positive results from lymph nodes and thyroid nodules
-Expensive
- Cannot be used in claustrophobic patient
24.
STANDARD BILATERAL EXPLORATION
•The neck is explored via a 3- to 4-cm incision just caudal to the cricoid
cartilage following which platysma and deep cervical fascia are openend
• After the strap muscles are separated in the midline, one side of the neck
is chosen for exploration.
• dissection during a parathyroidectomy is maintained lateral to the
thyroid, making it easier to identify the parathyroid glands and not
disturb their blood supply.
• . The middle thyroid veins are ligated and divided, thus enabling medial
and anterior retraction of the thyroid lobe, with the aid of a peanut
sponge or placement of 2-0 silk sutures into the thyroid.
25.
• The spacebetween the carotid sheath and thyroid is then opened by
gentle sharp and blunt dissection, from the cricoid cartilage superiorly
to the thy mus inferiorly and the RLN is identified.
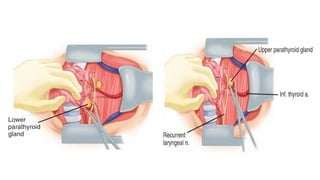
• Approximately 85% of the parathyroid glands are found within 1 cm of
the junction of the inferior thyroid artery and RLNs. The upper
parathyroid glands usually are superior to this junction and dorsal
(posterior) to the nerve, whereas the lower glands are located inferior
to the junction and ventral (anterior) to the recurrent nerve.
27.
• Parathyroid glandappear as caramel coloured structures.
• a suspicious nodule may be aspirated using a fine needle attached to
a syringe containing 1 cc of saline Very high PTH levels in the aspirate
have been shown to be diagnostic in the intraopera tive identification
of parathyroid glands
• size (>7 mm), weight, and color are used to distinguish normal from
hypercellular parathyroid glands. Hypercellular glands generally are
darker, more firm, and more vascular than normocellular glands.
28.
• If notfound at this location, the thyrothymic ligament and thymus should be mobilized. The
upper end of the cervical thymus is gently grasped with a right-angle clamp, and the distal
portion is bluntly dissected from perithymic fat with a peanut sponge.
• One can then “walk down” the thymus with successive right-angle clamps .Applying light
tension along with a “twisting” motion helps to free the upper thymus.
• The carotid sheath also should be opened from the bifurcation to the base of the neck if the
parathyroid tumor cannot be found.
• If these maneuvers are unsuccessful, an intrathyroidal gland should be sought by using
intraoperative ultrasound, incising the thyroid capsule on its posterolateral surface, or by
perform ing an ipsilateral thyroid lobectomy.
• Preoperative or intraoperative ultrasonography can be useful for identifying intrathyroidal
parathyroid glands. Rarely, the third branchial pouch may maldescend and be found high in
the neck (undescended parathymus), anterior to the carotid bulb, along with the missing
parathyroid gland. Upper para thyroid glands are more consistent in position and usually are
found near the junction of the upper and middle thirds of the gland, at the level of the cricoid
cartilage. Ectopic upper glands may be found in carotid sheath, tracheoesophageal groove,
retroesophageal, or in the posterior mediastinum
29.
• A singleadenoma -The adenoma is dissected free of surrounding
tissue
• Two abnormal and two normal glands are identified, the patient has
double adenomas. Triple adenomas are pres ent if three glands are
abnormal and one is normal- The abnormal glands should be excised,
provided the re maining glands are confirmed as such, thus excluding
asymmetric hyperplasia after biopsy and frozen section.
• All parathyroid glands are enlarged or hypercellular – subtotal
thyroidectomy or total parathyroidectomy with autotransplantation of
aroung 30 to 50gm of parathyroid tissue in forearm.
30.
MIAMI protocol
• The“Miami” criteria developed by Irvin and colleagues describe
biochemical cure as a 50% decrease in PTH levels from baseline 10 to
15 minutes after resection of the targeted parathyroid gland
31.
PARATHYROID CARCINOMA
• Themajor diagnostic criteria include vascular or capsular invasion,
trabecular or fibrous stroma, and frequent mitoses.
• neck explora tion, with en bloc excision of the tumor and the ipsilateral
thy roid lobe, in addition to the removal of contiguous lymph nodes
(tracheoesophageal, paratracheal, and upper mediastinal).
• The recurrent nerve is not sacrificed unless it is directly involved with
tumor. Adherent soft tissue structures (strap muscles or other soft tissues)
should also be resected.
• Modified radical neck dissection is recommended in the presence of
lateral lymph node metastases. Prophylactic neck dissection is not advised
• Endoscopic Parathyroidectomy
•minimally invasive, video-assisted parathyroidectomy techniques
(MIVAPs) are available that differ based on location of incisions—
cervical, transaxillary, transthoracic, or retroauricular.
34.
OUTCOMES AFTER PARATHYROIDSURGERY
• Biochemical cure is defined as normocalcemia after parathyroidsurgery that
lasts at least 6 months postoperatively
• Manifestations of RLN injury range from variable hoarseness in cases of
unilateral injury to severe airway compromise in cases of bilateral nerve
injury.
• Bleeding or Hematoma
• Postoperative Hypocalcemia - patients with significant, prolonged
postoperative hypocalcemia,rapid administration of intravenous calcium
gluconate is warranted this is accomplished by diluting 10 ampules of
calcium gluconate in 1 liter of normal saline. The initial infusion rate of 30
mL/hr is titrated, based on symptoms and serial serum calcium levels.