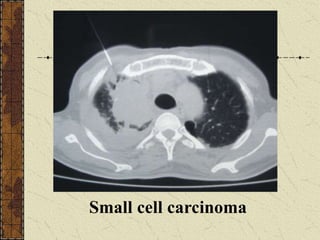
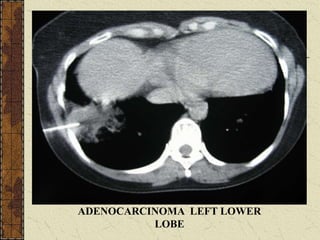
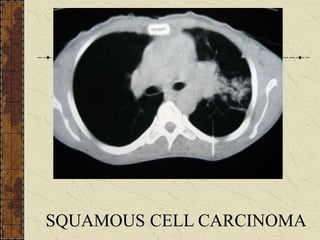
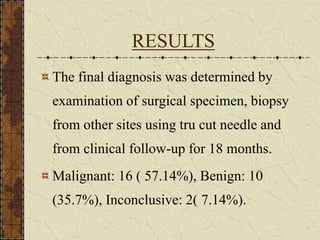
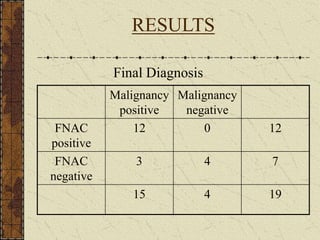
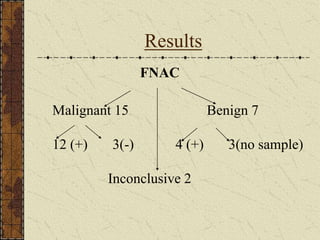
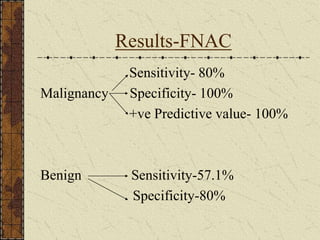
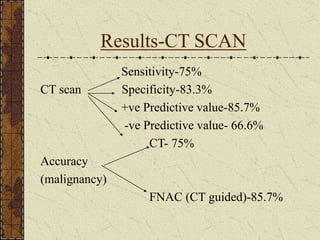
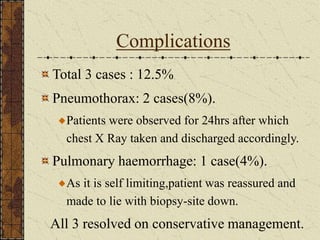
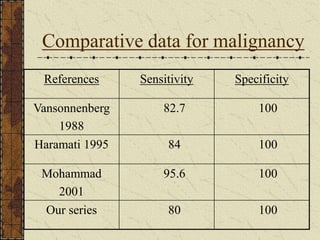
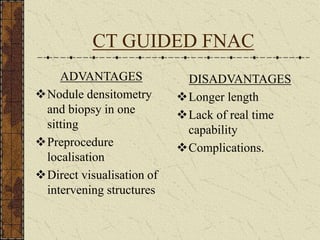
CT guided FNAC is a simple and effective technique for diagnosing complex pulmonary lesions. In a study of 28 patients, CT guided FNAC had a sensitivity of 80% and specificity of 100% for diagnosing malignancy. CT scanning alone had sensitivity of 75% and specificity of 83.3% for malignancy. Complications occurred in 3 patients (12.5%) and were minor and resolved with conservative treatment. The study concluded that CT guided FNAC is a highly sensitive and specific technique for characterizing pulmonary lesions.







































![FNAC_DIRECT_and_GUIDED Pathology [1]_FINAL2.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fnacdirectandguided1final2-260109235635-59e75d7d-thumbnail.jpg?width=640&height=640&fit=bounds)

















































