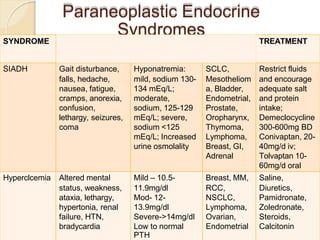
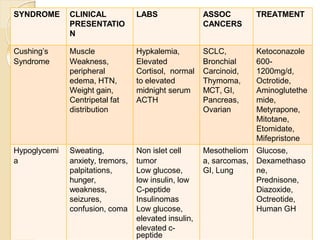
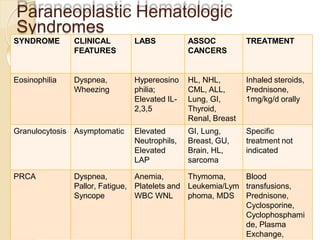
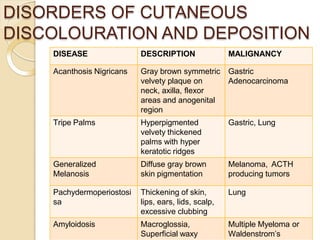
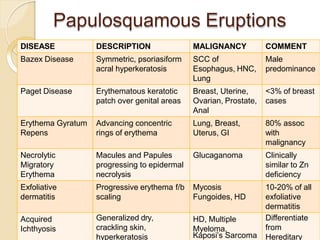
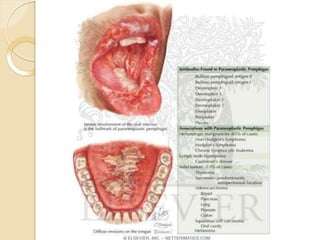
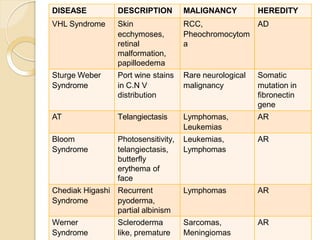
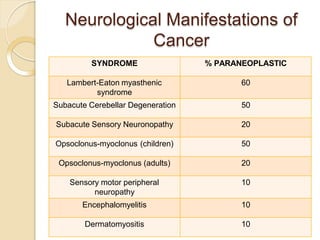
This document discusses paraneoplastic syndromes, which are clinical disorders associated with but not directly caused by malignant tumors. It provides examples of various paraneoplastic syndromes involving the endocrine system, hematologic system, skin, kidneys, lungs and other organs. It also discusses neurological manifestations such as opsoclonus-myoclonus syndrome, limbic encephalitis, cerebellar degeneration and others. Evaluation and treatment of the underlying malignancy is important for managing paraneoplastic syndromes.