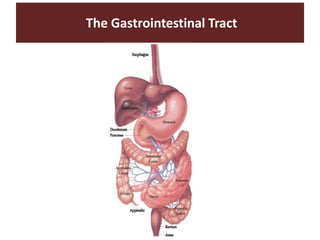
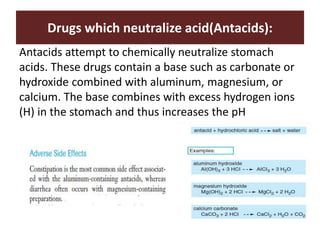
This document discusses drugs used to treat gastrointestinal disorders. It begins by outlining the objectives and anatomy of the gastrointestinal tract, including the cells and glands of the stomach that secrete hydrochloric acid and enzymes. Common acid-related diseases like ulcers and GERD are then described. The rest of the document focuses on classes of drugs used to treat these conditions, including antacids, mucosal protective agents, proton pump inhibitors, H2 receptor antagonists, and prostaglandins. The mechanisms of action and indications for specific drugs in each class are provided.