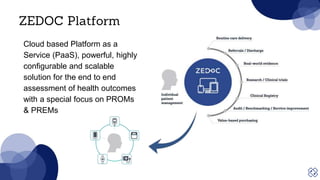
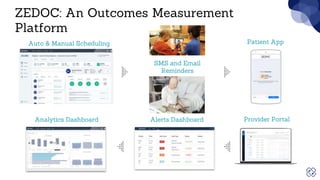
The document discusses strategies to overcome patient engagement barriers in healthcare, emphasizing the importance of patient-reported outcomes (PROs) and experience measures (PREMs) for improving health outcomes and communication. It outlines the Zedoc platform's features and methods for enhancing engagement, including personalized onboarding, minimizing respondent burden, and using behavioral analytics. Key takeaways highlight the significance of creating a human-centric approach and adapting methods based on patient feedback.