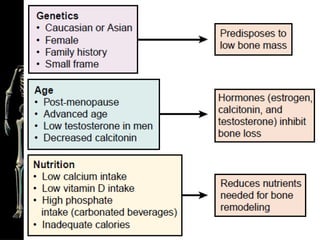
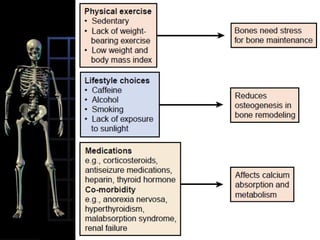
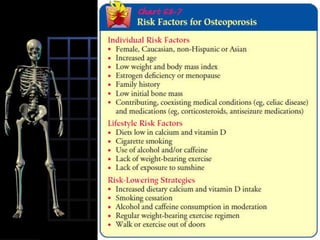






Osteoporosis is a metabolic bone disorder characterized by decreased bone mass and density, leading to porous and brittle bones that are prone to fracture. It is classified as either primary or secondary osteoporosis. Primary osteoporosis includes type I, which usually affects postmenopausal women, and type II, which occurs most commonly in those ages 70-85. Symptoms may include fractures after minor trauma. Diagnosis involves imaging tests to measure bone mineral density. Treatment focuses on controlling bone loss and preventing fractures through exercise, medication, supplements, and lifestyle changes. Nursing care emphasizes safety, mobility, nutrition, pain management, and education.










![Osteomalacia 2nd-150704155942-lva1-app6892 [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/osteomalacia-2nd-150704155942-lva1-app6892autosaved-200520081743-thumbnail.jpg?width=640&height=640&fit=bounds)



















































































