Downloaded 70 times


![DONESUMAB[RANKL INHIBITOR]
Dose- 60mg every 6months S.C
Used in postmenopausalwomen.](https://image.slidesharecdn.com/osteoporosisppt-190815143421/85/Osteoporosis-51-320.jpg)
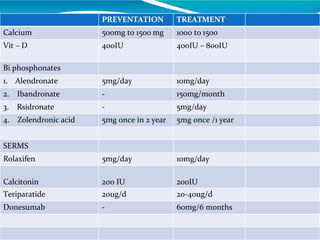

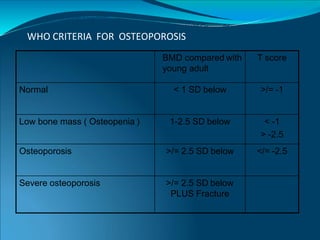
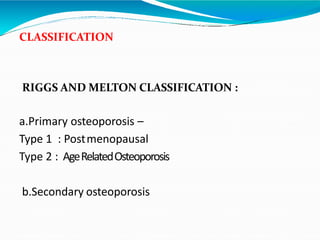
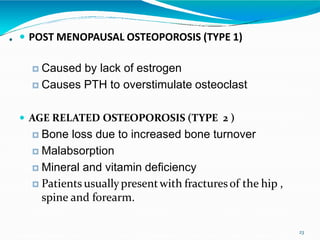
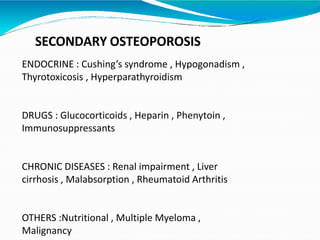
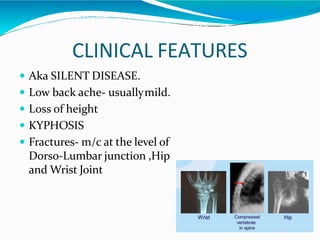
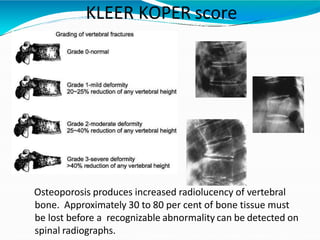
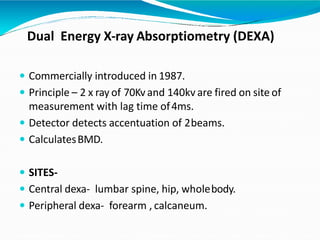
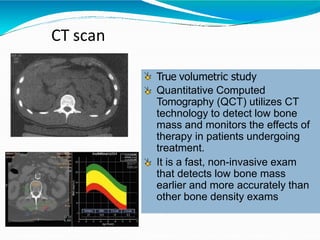
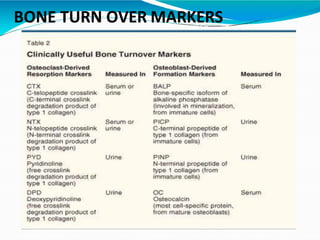
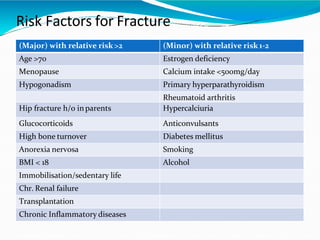
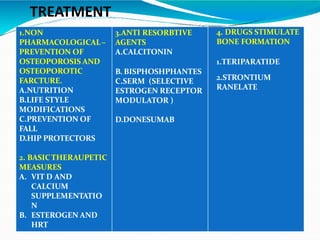
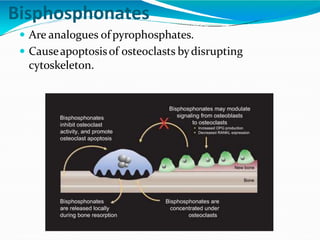
This document provides information on osteoporosis, including its definition, classification, epidemiology, clinical features, investigations used for diagnosis, and management. Osteoporosis is defined as a reduction in bone density leading to an increased risk of fractures. It is classified based on whether it is primary/secondary and type. Diagnosis involves tests like DEXA scans, biomarkers, and imaging. Management includes lifestyle modifications, calcium/vitamin D supplementation, and medications like bisphosphonates, teriparatide, and denosumab that reduce resorption or stimulate bone formation.























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















