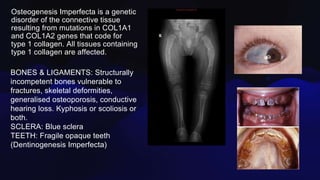
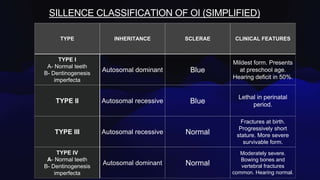
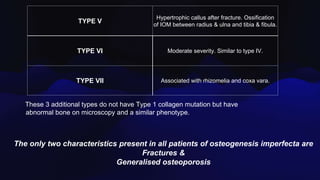
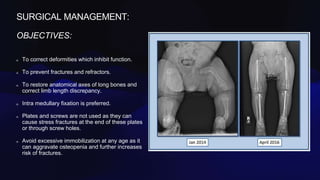
Osteogenesis imperfecta is a genetic disorder caused by mutations in COL1A1 and COL1A2 genes affecting type 1 collagen. It is characterized by fragile bones that fracture easily, skeletal deformities, blue sclera, and dentinogenesis imperfecta. There are several classifications of OI based on inheritance, clinical features, and severity. Management involves medications like pamidronate to increase bone density and reduce fractures, bracing and surgery to correct deformities, and physical therapy to aid mobility. Genetic testing can confirm the diagnosis.















![Osteogenesis Imperfecta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/osteogenesisimperfectaautosaved-230505163031-62b018a2-thumbnail.jpg?width=640&height=640&fit=bounds)




























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



