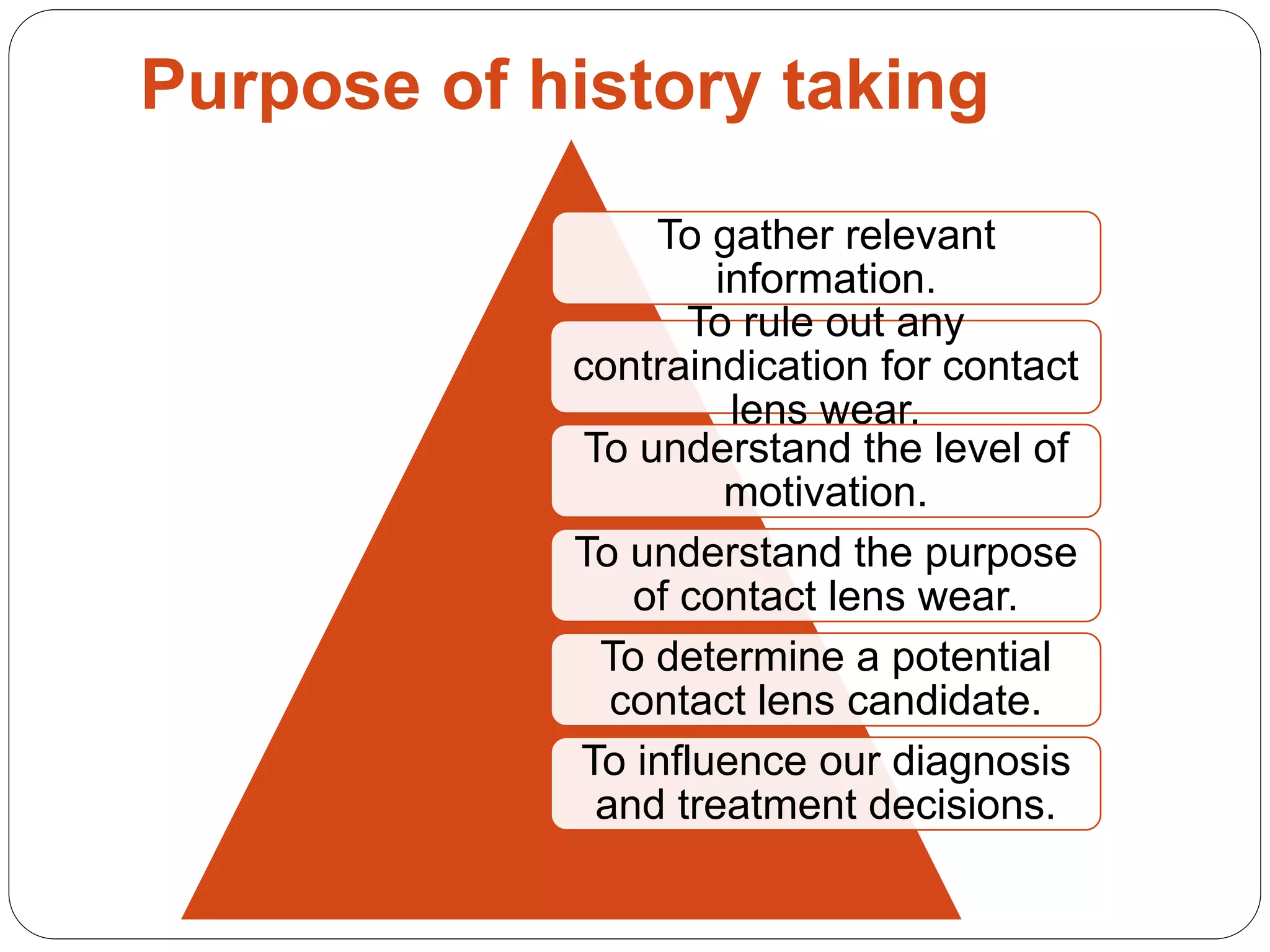
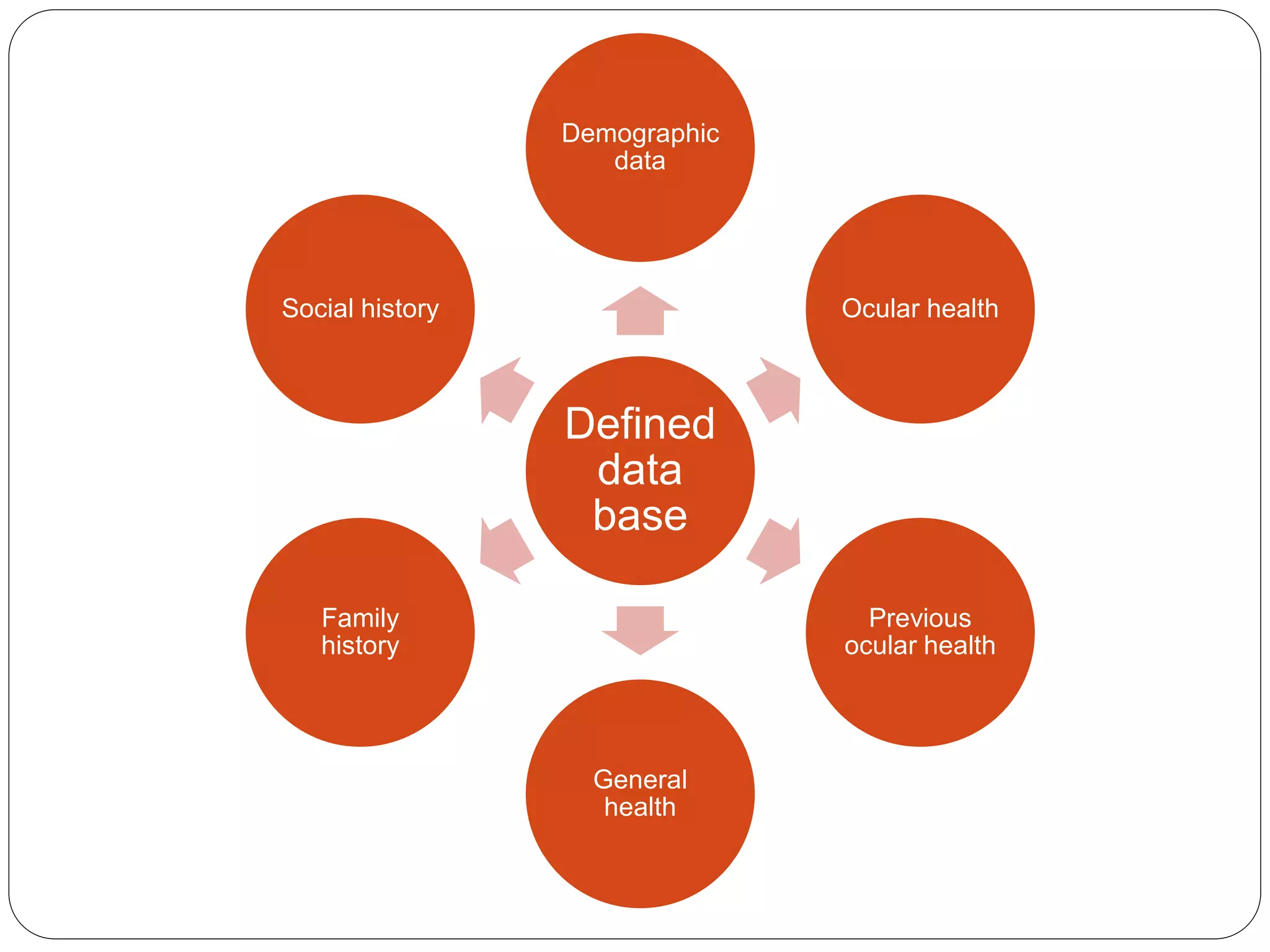
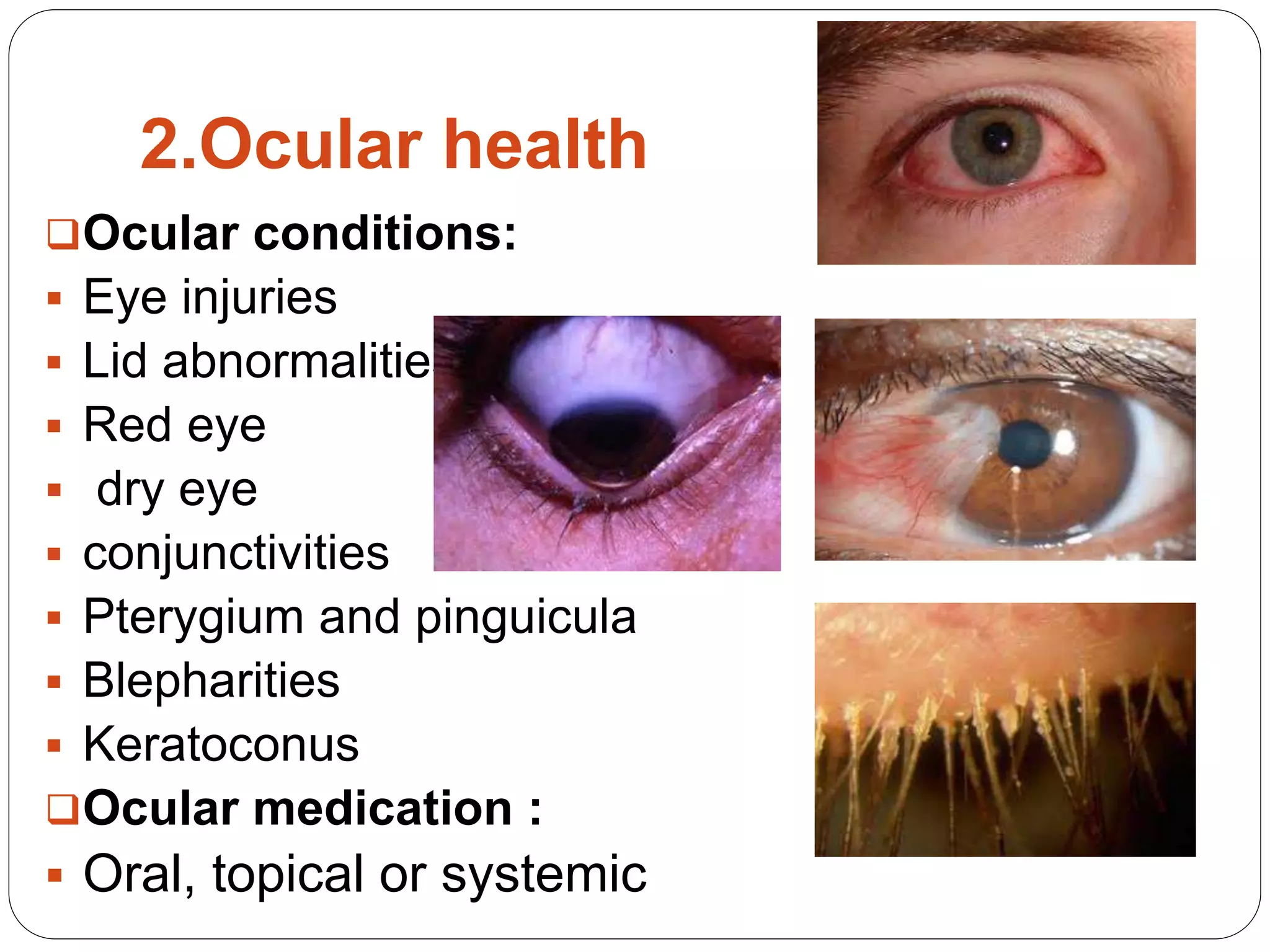
The document discusses the importance and process of history taking for contact lens fitting. It outlines the key components of a thorough history, including demographic data, ocular health history, general medical history, medication use, family history, social history, and history of prior contact lens use. A complete history is essential to identify any contraindications, determine the appropriate lens type, and manage patient expectations. Experts emphasize that the patient's history is one of the most important tools for optometrists and can often lead directly to a diagnosis.