Download to read offline



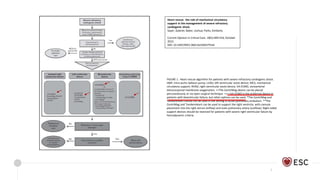
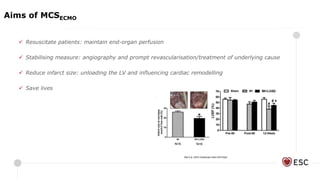
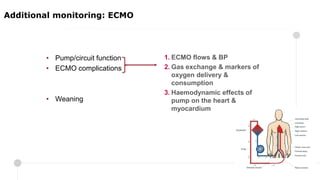



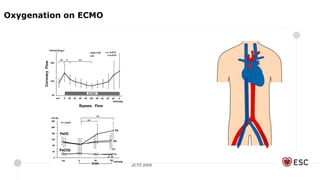
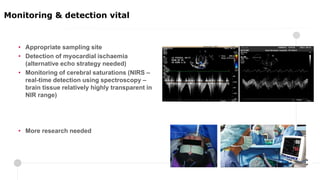
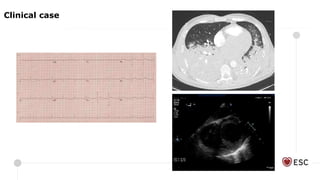

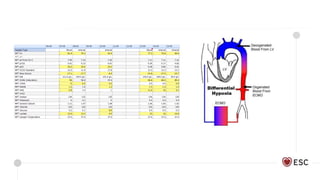

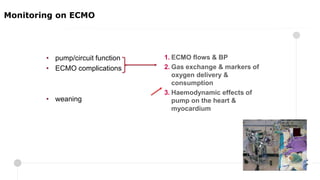
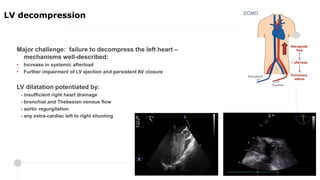
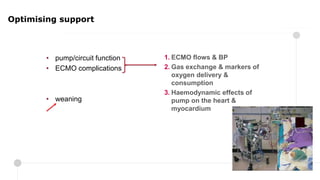



This document discusses optimizing extracorporeal membrane oxygenation (ECMO) support. It begins by outlining the goals of ECMO as resuscitating patients, reducing infarct size, and saving lives. It then discusses standard and additional monitoring needed on ECMO, potential obstructions like thrombus, and optimizing gas exchange. Finally, it covers monitoring the haemodynamic effects of ECMO on the heart, decompressing the left ventricle, and determining readiness for weaning a patient off ECMO support.


![Anaesthesia for cardiopulmonary bypass surgery [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anaesthesiaforcardiopulmonarybypasssurgeryautosaved-150531185352-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)



![Clinicalteaching [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalteachingautosaved-180718063103-thumbnail.jpg?width=640&height=640&fit=bounds)










































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





