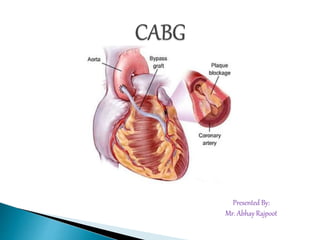
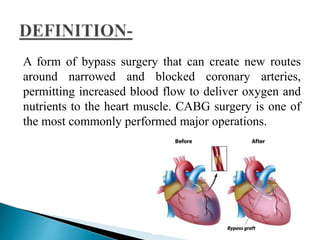


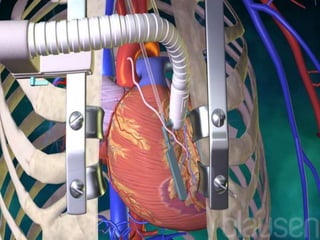





Coronary artery bypass graft (CABG) surgery is performed to bypass blocked coronary arteries and improve blood flow to the heart. The document describes the procedure, which involves harvesting blood vessels such as the internal mammary artery to bypass narrowed arteries. First performed in India in 1975, over 60,000 CABG surgeries are now performed annually. The pre-operative, intra-operative and post-operative process is outlined, including indications, risks, and benefits of CABG surgery.























































































