Downloaded 210 times
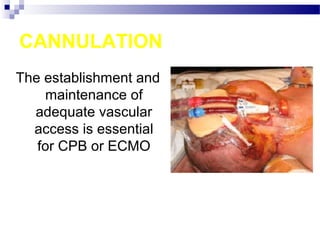
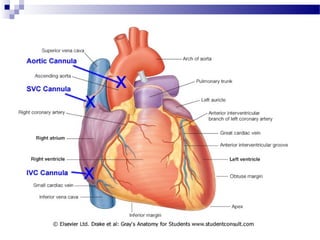
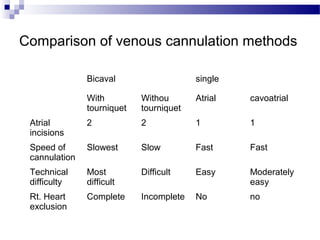
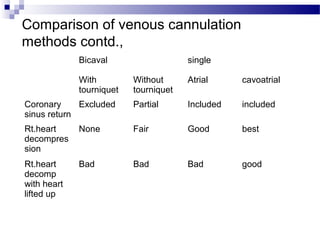
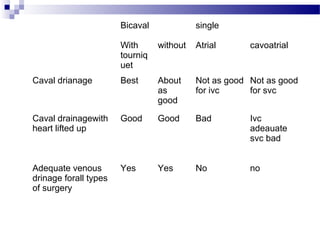
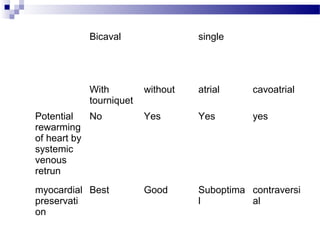
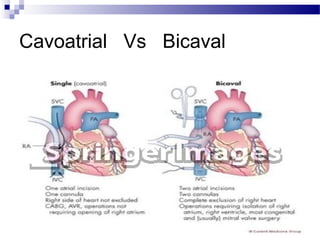
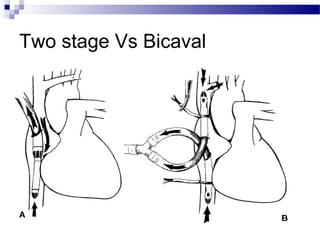


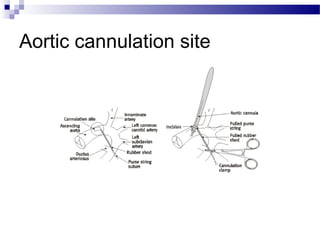


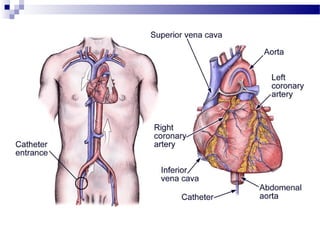
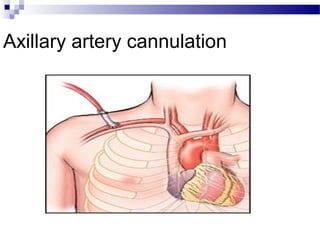
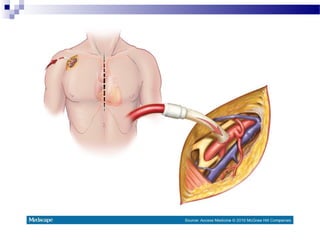

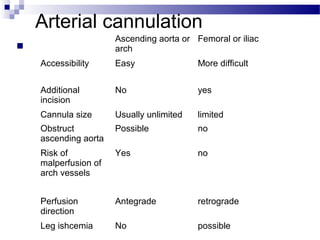
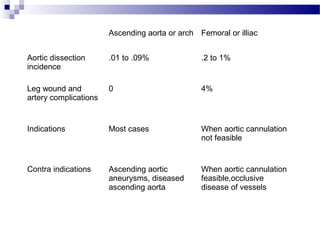

The document discusses various techniques for cannulation during cardiopulmonary bypass (CPB). Venous cannulation is typically done via the superior vena cava (SVC) and inferior vena cava (IVC) using either a bicaval, single atrial, or cavoatrial approach. Arterial cannulation is usually via the ascending aorta but can also be done through femoral, axillary, or other arteries if needed. Proper positioning and sizing of cannulas is important to maximize blood flow and minimize complications like air embolism, bleeding, or malposition. Factors such as patient anatomy, surgical plan, and vessel disease must be considered to select the optimal cannulation method.












































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










