Downloaded 66 times

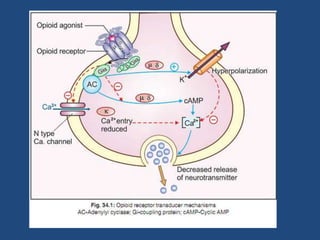







The document discusses opioids such as morphine, codeine, pethidine, fentanyl and methadone. Morphine is described as the prototype opioid analgesic that acts primarily on the central nervous system to produce analgesia, sedation, euphoria and respiratory depression. It also causes constipation, nausea, vomiting and hypotension. Tolerance develops to morphine's effects except for miosis and constipation. Pethidine causes less respiratory depression and histamine release compared to morphine. Fentanyl is 80-100 times more potent than morphine. Methadone has a high oral bioavailability and prolonged duration of action. Opioids are used for pain relief, pre-anesthesia