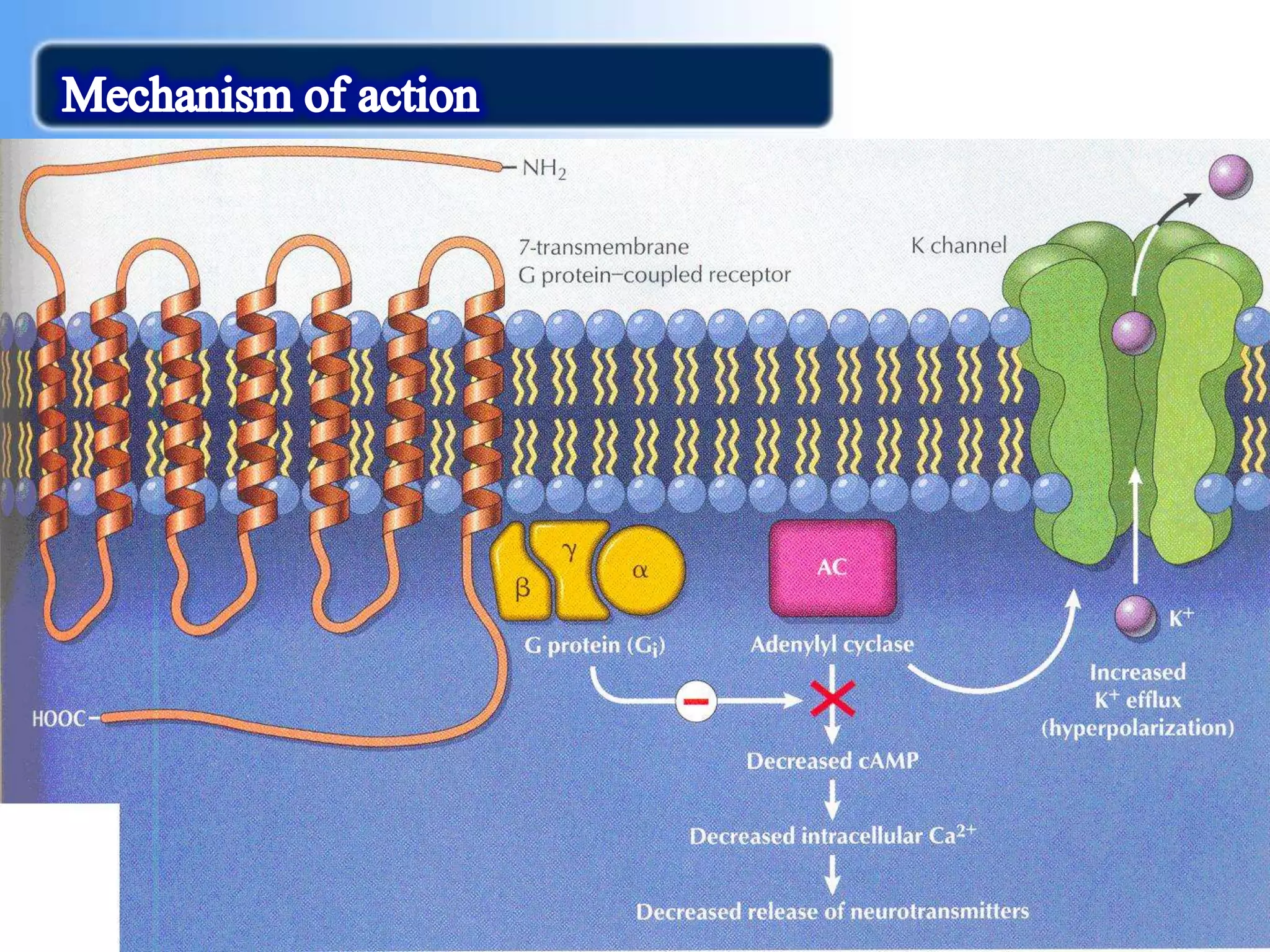
Morphine is a potent opioid analgesic that was first isolated from opium in 1805. It acts primarily on mu-opioid receptors in the central nervous system to powerfully suppress pain. While very effective for treating severe pain, morphine also carries risks of respiratory depression, physical dependence, and accidental overdose that can cause death. It was the first opioid analgesic to be widely used medicinally but also misused criminally, such as in one of the earliest recorded homicides involving morphine poisoning in 1823.