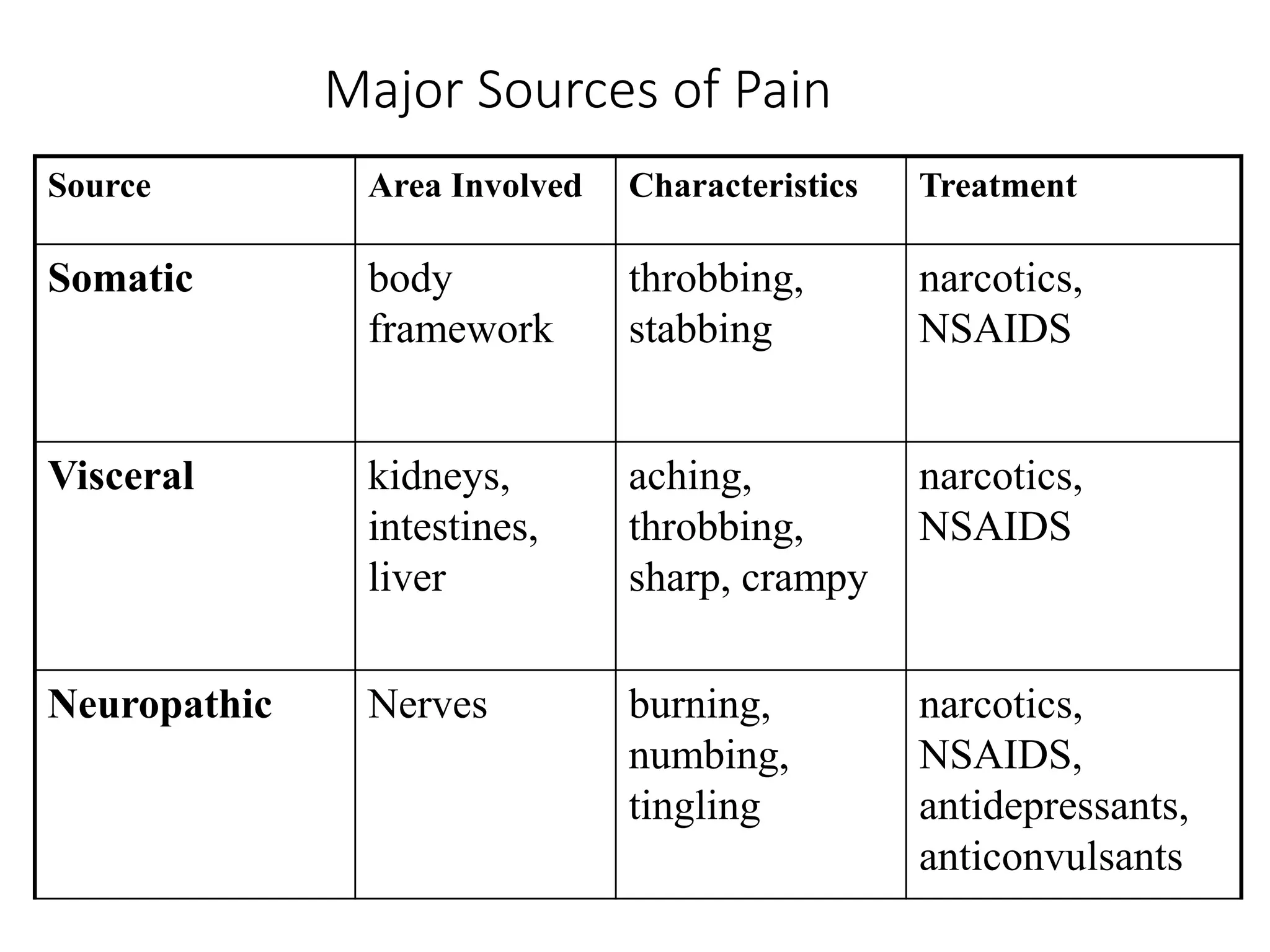
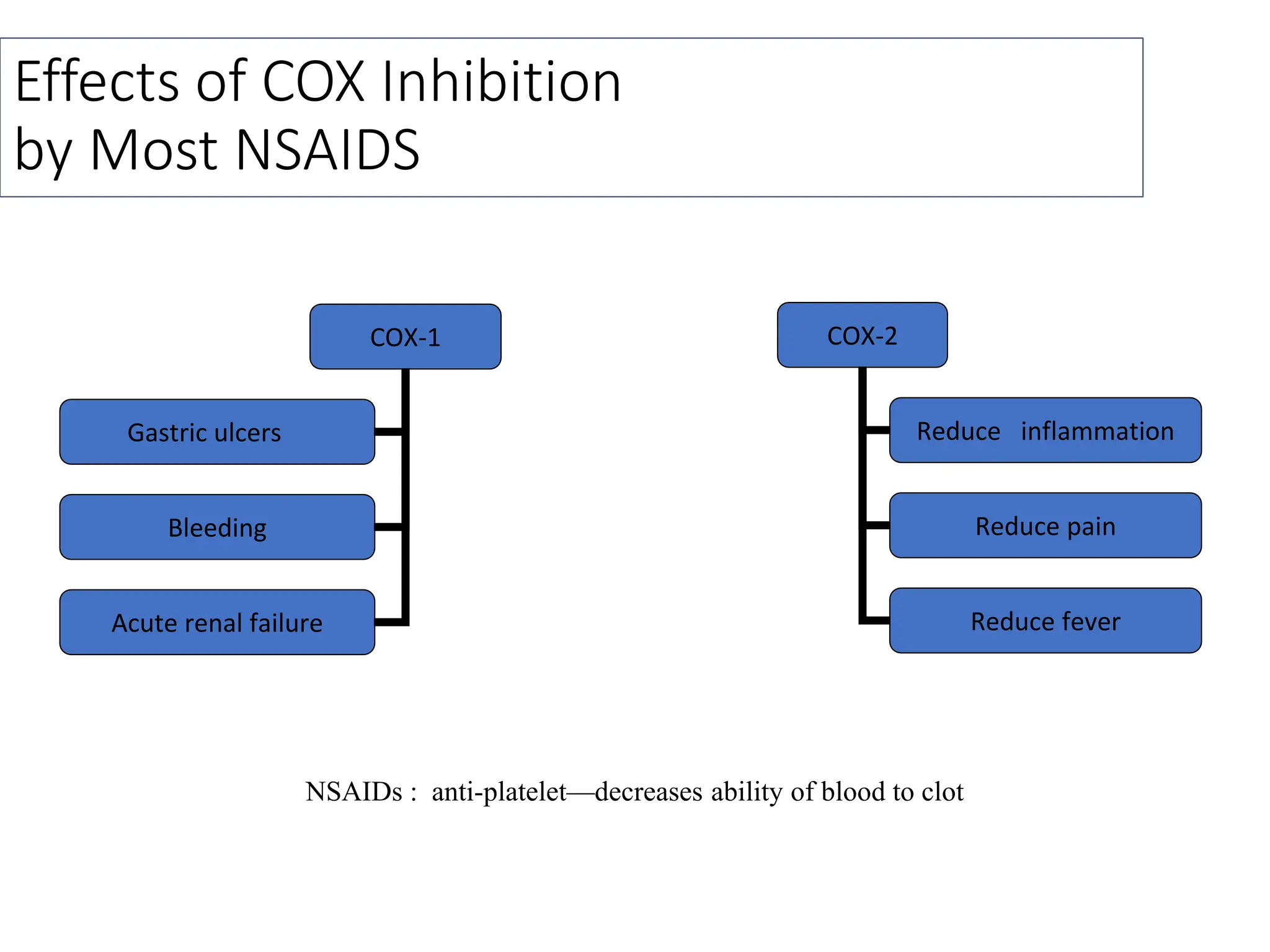
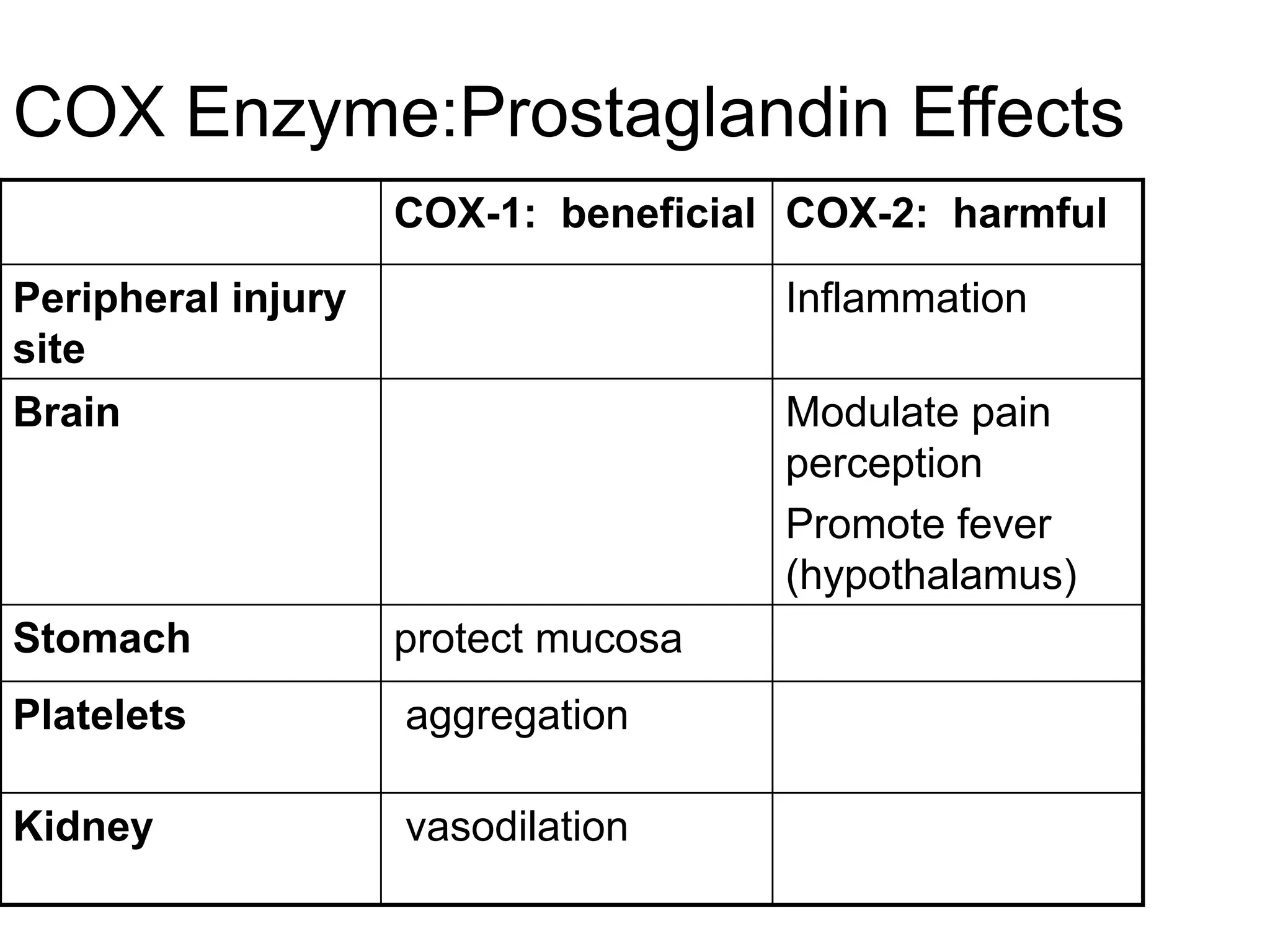
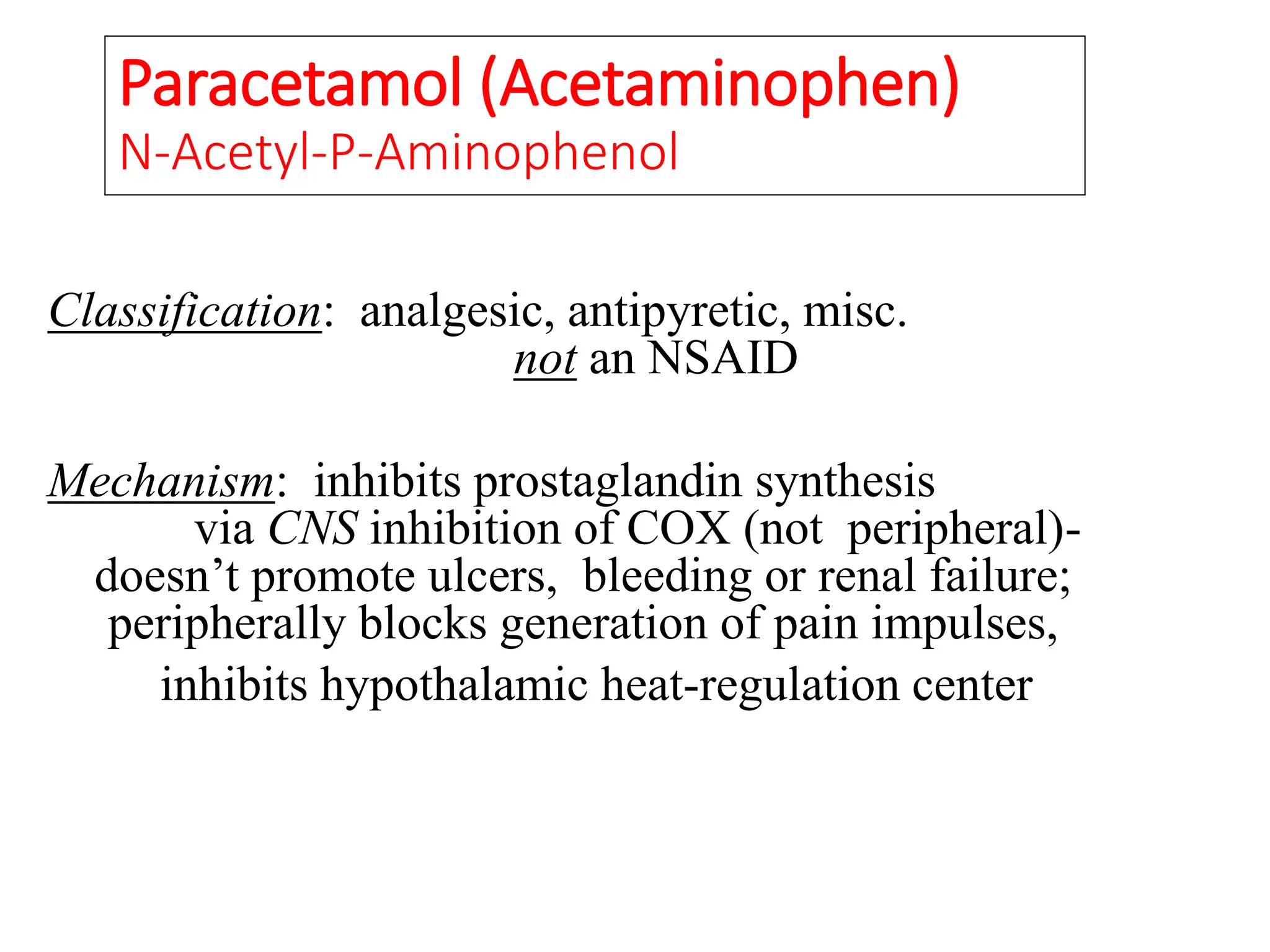
This document provides an overview of analgesics, including both opioid and non-opioid analgesics. It discusses various opioid analgesics like morphine, codeine, fentanyl and pentazocin. It describes their mechanisms of action, indications, routes of administration, side effects and contraindications. It also discusses non-opioid analgesics like paracetamol, acetylsalicylic acid and analgin, and describes their mechanisms of action as inhibitors of prostaglandin synthesis. The document classifies different types of pain and summarizes the history and development of commonly used opioid analgesics.






























































![100013603 [Repaired] [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/100013603repairedauto-saved-240104174437-00157480-thumbnail.jpg?width=640&height=640&fit=bounds)






























