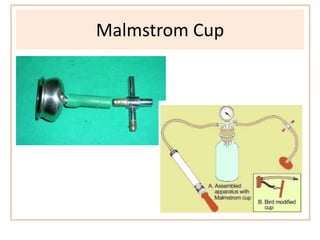
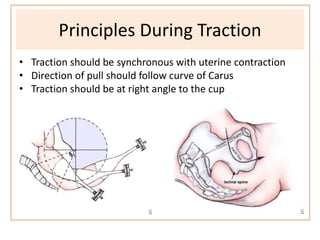
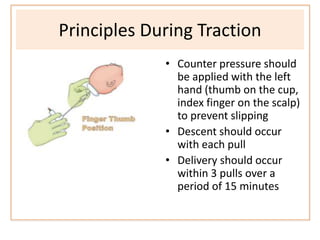
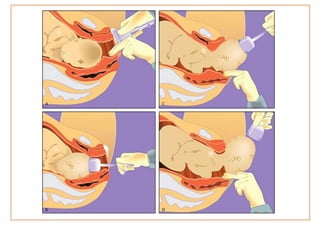
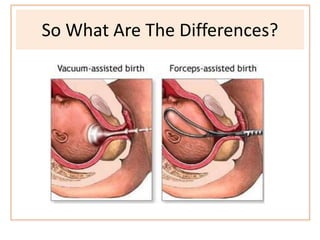
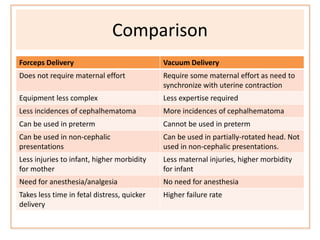
Vacuum delivery is a device used to assist delivery by creating negative pressure between a suction cup and the fetal scalp. It has a suction cup, vacuum generator, and traction tubing. There are different cup types, including Malmstrom, Bird, and soft silicone cups. Vacuum delivery is indicated for maternal or fetal distress in the second stage of labor or prolonged second stage. Proper technique involves assessing fetal position, applying the cup to the flexion point, gradually increasing negative pressure, and applying traction in sync with contractions along the curve of Carus. Complications can include cephalhematoma and injuries for the baby or soft tissue injuries for the mother.