The hadith advises against suspicion, spying, listening to gossip, and having enmity with others. It encourages people to be brothers and avoid these false and harmful behaviors.
Hazrat Abu Hurairanarrated
The Prophet (PBUH) said,
“Beware of suspicion( about others)
as suspicision is the falsest talk,
and do not spy upon each other,
and do not listen to the evil talk of
people about other’s affairs
and do not have enemity with one
another but be brothers”
Bukhari Book#62 Hadith# 74
4.
Outline
What isan odontogenic tumor
Odontogenic tissues giving rise to
tumors
Classification
Clinical, radiographic and
histopathological features
Take home message
5.
WHAT IS ATUMOR?
Abnormal growth of tissue resulting from
uncontrolled progressive multiplication
of cells, serving no physiologic function.
ODONTOGENIC TUMOR?
Tumor arising from odontogenic tissue.
6.
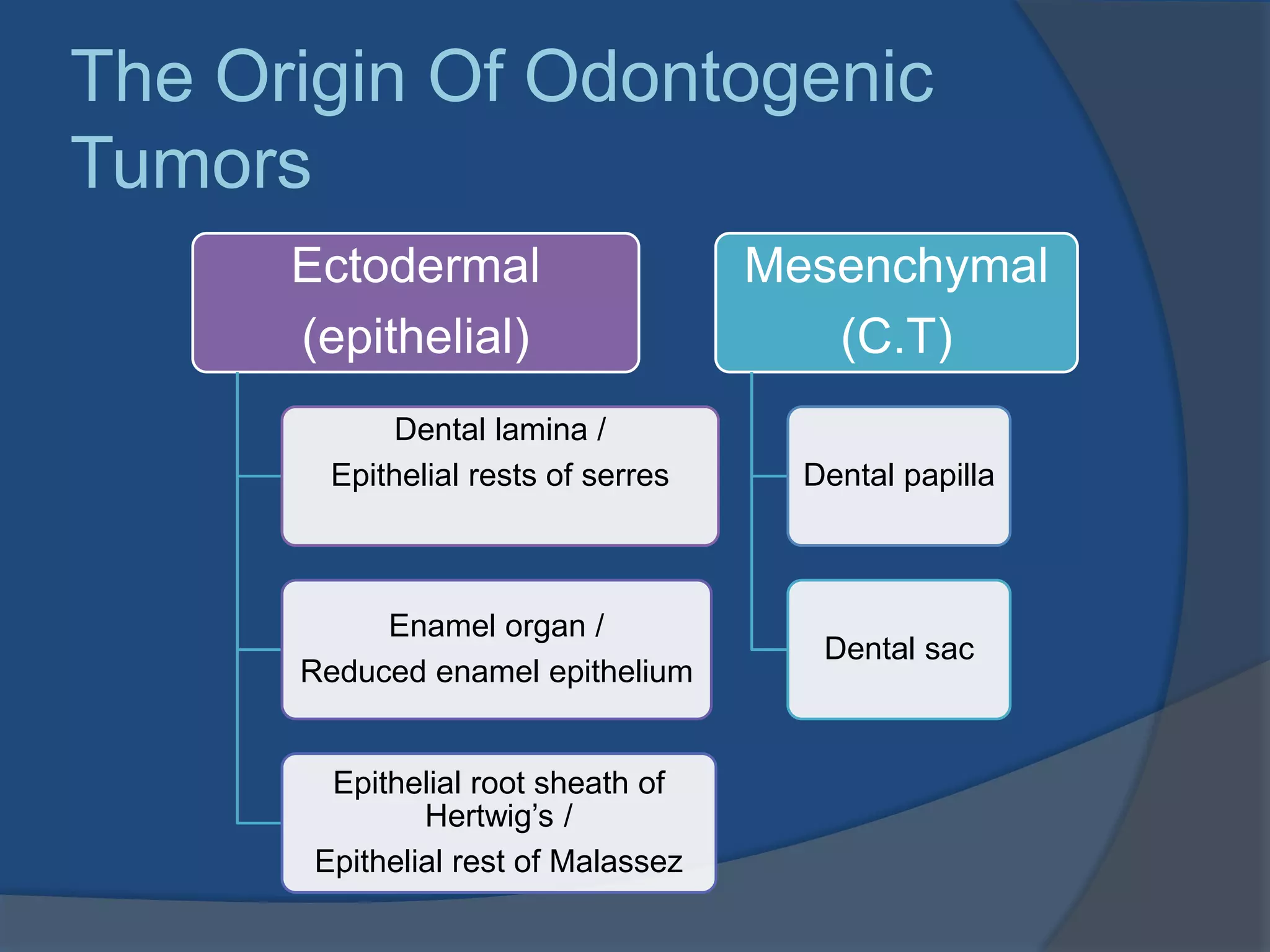
The Origin OfOdontogenic
Tumors
Ectodermal
(epithelial)
Dental lamina /
Epithelial rests of serres
Enamel organ /
Reduced enamel epithelium
Epithelial root sheath of
Hertwig’s /
Epithelial rest of Malassez
Mesenchymal
(C.T)
Dental papilla
Dental sac
Locally aggressive neoplasmof odontogenic epithe-
-lium that has a wide spectrum of histologic
pattern resembling early odontogenesis.
1. Dental lamina/Rest of serres
2. Enamel organ/Reduced enamel epithelium
3. Basal layer of oral mucosa
4. Epithelial lining of dentigerous cyst
Painless nonulcerated, sessile or
pedunculated masses in gingival or
alveolar mucosa.
Some lesions may cause superficial
bone erosion.
Histological features are same as
intraoseous Ameloblastoma.
23.
Solid Ameloblastomaare treated with block
excision or resection followed by
immediate reconstruction.
Margin of resection 1-1.5 cm past
radiographic margins.
Luminal and intraluminal Enucleation
Intramural resection with peripheral
osteotomy
Perioheral types conservative local
excision
Ameloblastic CA and Malignant A treated
more aggressively but prognosis is v poor.
Patients should be followed indefinitely.
Resection
Removal of tumorby incising
through uninvolved tissue around the
tumor.
Marginal resection; bony continuity not
disrupted
Partial resection; portion of jaw is removed
creating a continuity defect
Total resection; Complete bone is removed
with tumor, e.g mandibulectomy
Composite resection; tumor resection with
bone, soft tissue and lymph channels.
26.
CEOT ( PINDBORG
TUMOR)Cellsof origin unknown, dental lamina remnants
and stratum intermedium suggested.
Clinical features
•Mean age 40 yrs
•Mandible> maxilla
•Molar-ramus area
Radiographic features
•Unilocular or multilocular giving
honeycomb appearance
•May be complete radiolucent or
may contain small opacities
•Well circumscribed but sclerotic
margins may not always be
seen.
27.
HISTOPATHOLOGY
•Large polyhedral cellsin a fibrous stroma
•Nucei show considerable variation in size and
shape
•Extracellular amyloid of epithelial origin typical
of these tumors.
Liesegang rings
•Concentric calcific
rings with annular
staining pattern
seen in amyloid
material.
28.
TRAETMENT
Conservative localresection with a
narrow rim of surrounding bone is
treatment of choice.
Recurrence 15%
Rare malignant transformation
29.
Probably originates from
reducedenamel epithelium
Clinical features;
Teenagers mostly
affected
F>M
Anterior portion of jaws
Maxilla>mandible
Associated with crown
of an impacted tooth
Adenomatoid OT
Radiographic features;
Folliclar;Well circumscribed unilocular
lesion, around the crown of an impacted
tooth.
Extrafolicular; Same but appear above,
between or superimposed over roots of
an unerupted tooth.
Small opaque foci are distributed
throughout the lesion.
SQUAMOUS ODONTOGENIC
TUMOR
Rare tumorthought to arise from dental lamina
rests or rests of Malassez.
Occurs over a wide age range and are randomly
distributed through mandible and maxilla.
Radiographically well circumscribed lucency
associated with cervical region of roots of
teeth.
Microscopically has some similarity to
ameloblastoma, but lacks peripheral columnar
palisaded layer.
36.
CLEAR CELL ODONTOGENIC
TUMOR(CARCINOMA)
Rare neoplasm
Origin is unknown but location and histology
suggests odontogenic origin
Usually found in women older than 60 years
Locally aggressive and poorly circumscribed
Metastasis to lungs and lymph nodes
Radical surgery is required and recurrence rates
upto 50% are reported.
37.
MESENCHYMAL TUMORS
ODONTOGENIC MYXOMA
Resemblesmicroscopically dental pulp or
follicular C.T.
Clinical features
Smaller asymptomatic, may cause bony
expansion.
More common in mandible
Mean age 30 yrs
38.
RADIOGRAPHIC
FEATURES
Unilocular or
Multilocularlucency
“ Soap bubble appe-
arance “
Margins are irregular
Lucent defect may
contain thin whispy
trabeculi of bone arr-
anged at right angle
to each other
“Stepladder pattern”
39.
HISTOPATHOLOGY
Cells arehaphazardly
distributed through
loose abundant
myxoid stroma
containing only few
collagen fibrils.
Bony islands
40.
TREATMENT
Surgical excisionis treatment of choice
Due to lack of encapsulation recurrence
rates are high if treated conservatively.
41.
CENTRAL ODONTOGENIC
FIBROMA
Raretumor, more common in females
Aprox 45% occur anterior to 1st molar
region in maxilla.
Usually appears as multilocular
radiolucency causing bony expansion.
Surgical excision or enucleation is
traetment
Recurrence is rare
42.
CEMENTOBLASTO MA/ TRUE
CEMENTOMA
Rare benign neoplasm of cementoblasts
Microscopically resembles
osteoblastoma but is connected or fused
to the root of a tooth.
More common in posterior mandible
Radiographically it is an opaque tumor,
usually surrounded by thick, uniform
radiolucent ring, contiguous with PDL
space.
43.
MIXED TUMORS
Ameloblastic Fibromaand Fibro-odontoma
Except for presence of odontoma both are same
and considered together…
Clinical Features;
Younger age group mean 12yrs
F=M
Mandibular molar area is favoured location
Commonly asymptomatic
44.
Radiographic
features
Well circumscribedwith
sclerotic margins
Unilocular/ multilocular
AF complete radiolucent,
AFO opaque focus
appears
May be associated with
crown of impacted tooth
45.
HISTOPATHOLOGY
Fibrous capsule
Myxoid C.T
Evenly distributed
strands of epithelium
In fibro-odontoma
one or more foci
containing enamel,
dentine and
cementum are found
46.
TREATMENT
Because of encapsulationand general
lack of invasive capacity treated through
conservative surgical approaches like
curettage or excision.
Rare malignant counterpart Mlignant
Ameloblastic Fibrosarcoma has been
reported
47.
ODONTOMA
Most common odontogenictumor
Biologicaly may be considered as
Hamartomas, composite of enamel and
dentine.
Compound Odontoma;
Miniature or rudimentary teeth.
Complex odontoma;
Amorphous conglomeration of hard
tissue.
Hamartoma;
Excess of normaltissue in normal
location, e.g odontomas
Choristoma;
Excess of normal tissue in abnormal
location e.g osseous choristomas in
tongue
50.
Clinical Features
Histopathology
Youngeradults
Maxilla > mandible
Compound O more
common in anterior
Complex O more
common in posterior
regions
Mostly associated
with impacted or
retained tooth
Normal appearing
enamel, dentine,
pulp or cementum
may be seen
TAKE HOME MESSAGE
Most of the bony tumors of mandible
and maxilla have odontogenic origin.
Clinical, radiographic and histopathology
correlation is required for diagnosis.
Excision is treatment of choice.