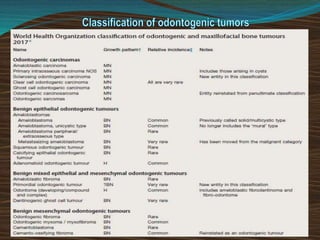
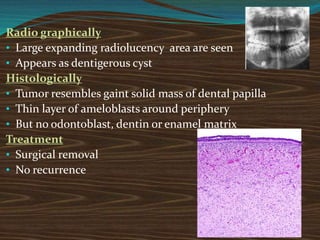
The document discusses several odontogenic tumors including:
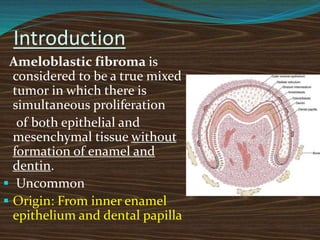
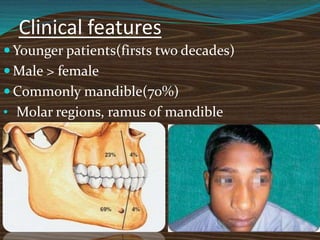
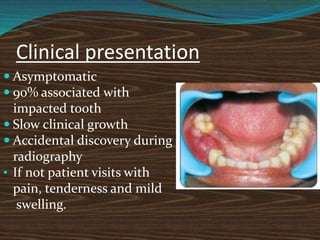
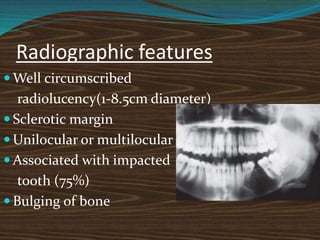
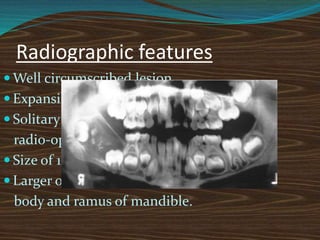
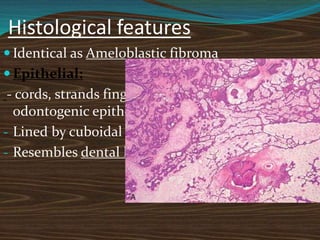
Ameloblastic fibroma is a mixed tumor of odontogenic origin composed of neoplastic epithelium and connective tissue that commonly occurs in children and teenagers. It is often associated with an impacted tooth.
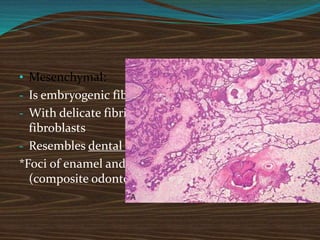
Ameloblastic fibro-odontoma is similar to ameloblastic fibroma but contains neoplastic epithelium, neoplastic myxomatous connective tissue, and foci of enamel and dentin formation.
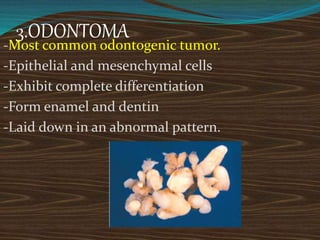
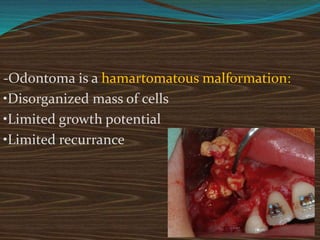
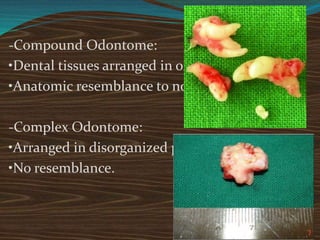
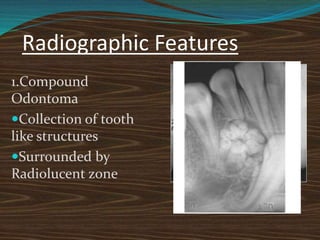
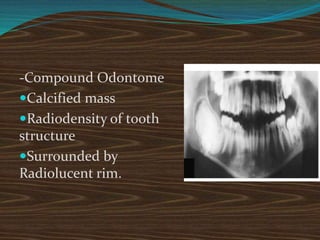
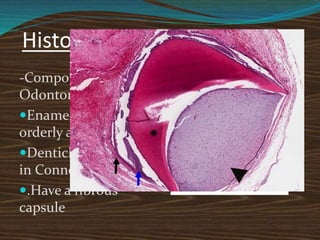
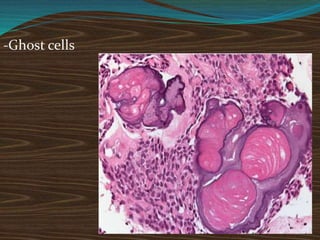
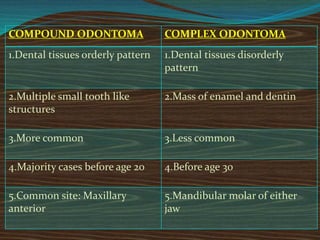
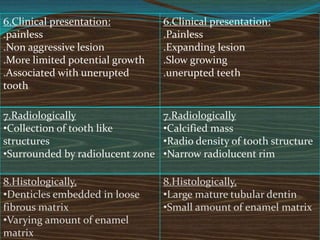
Odontoma is the most common odontogenic tumor and is considered a hamartoma. It has two types, compound and complex, which are composed of enamel and dentin laid down in an abnormal pattern












































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)