Downloaded 63 times


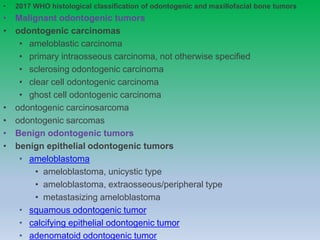
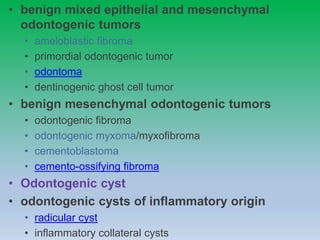
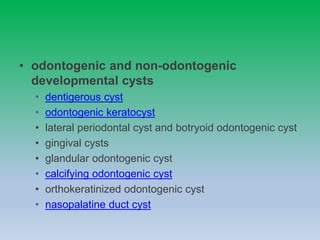
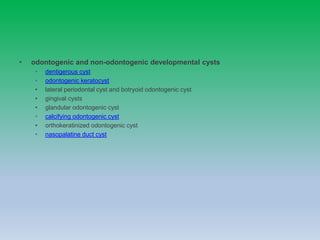

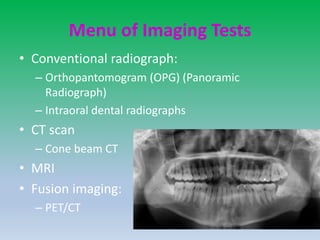
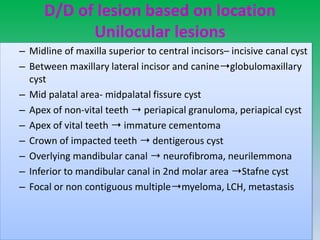
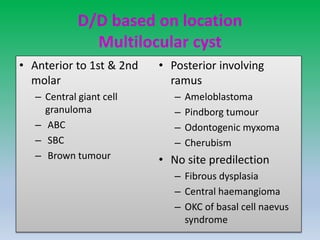
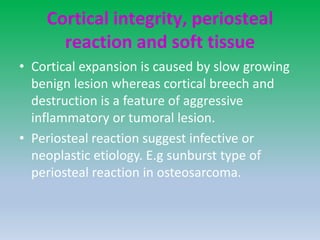
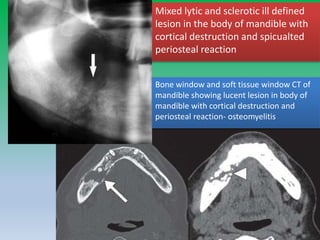














The document outlines the 2017 WHO histological classification of odontogenic and maxillofacial bone tumors, detailing various malignant and benign tumors, odontogenic cysts, and their characteristics. It discusses diagnostic imaging techniques to distinguish between conditions based on lesion margins, locularity, and effect on surrounding structures. Key odontogenic and non-odontogenic lesions are defined, with specific references to conditions like ameloblastoma, keratocystic odontogenic tumor, and various cystic lesions.




































![CystS in oral pathology dental edu[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cysts1-250430234019-1ab3f067-thumbnail.jpg?width=640&height=640&fit=bounds)
































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








