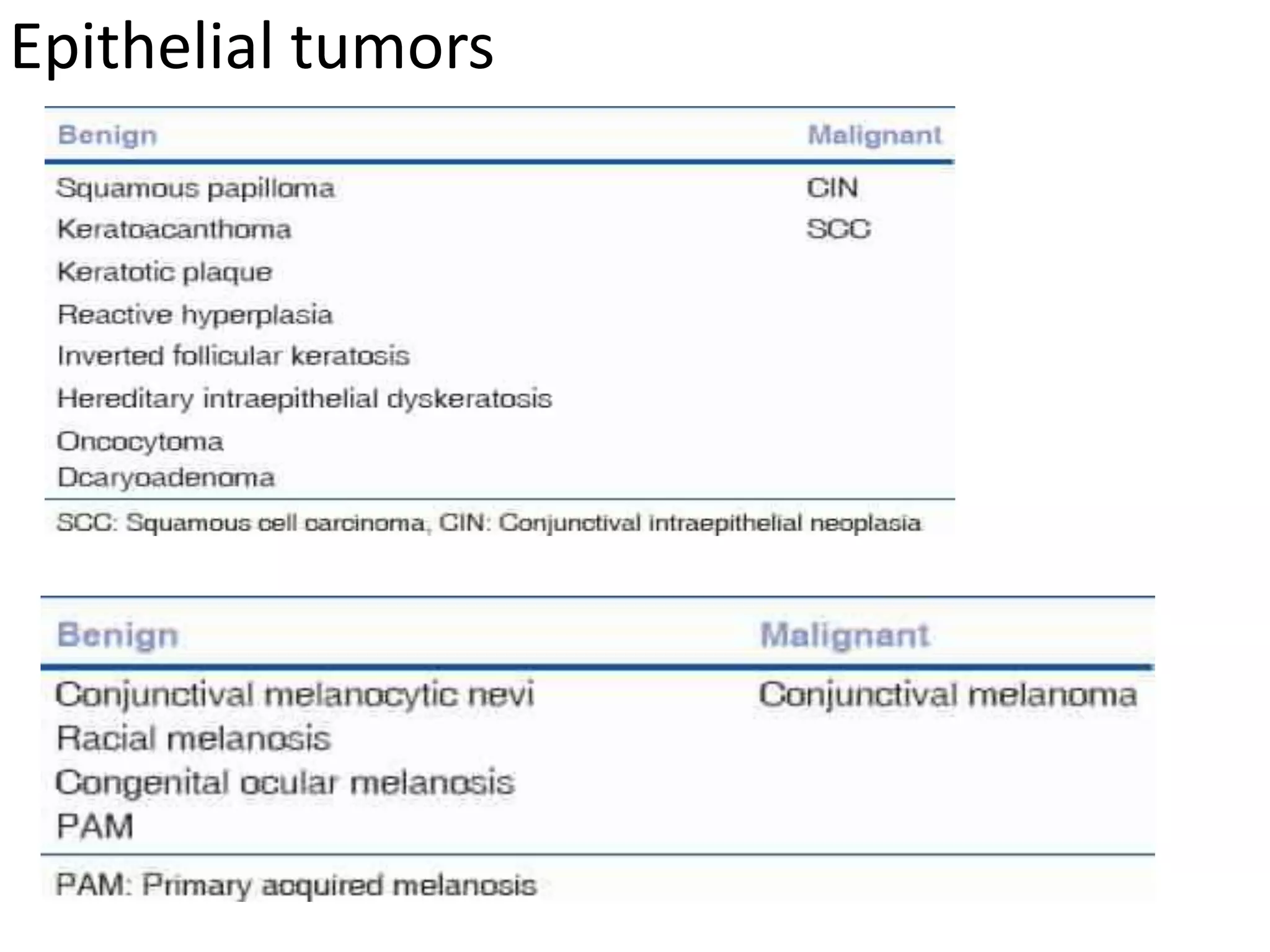
This document discusses ocular surface squamous neoplasia (OSSN), a term that encompasses precancerous and cancerous epithelial lesions of the conjunctiva and cornea. Some key points:
- OSSN accounts for 39% of all premalignant and malignant ocular surface lesions. Risk factors include ultraviolet light, immunosuppression, HPV infection, and smoking.
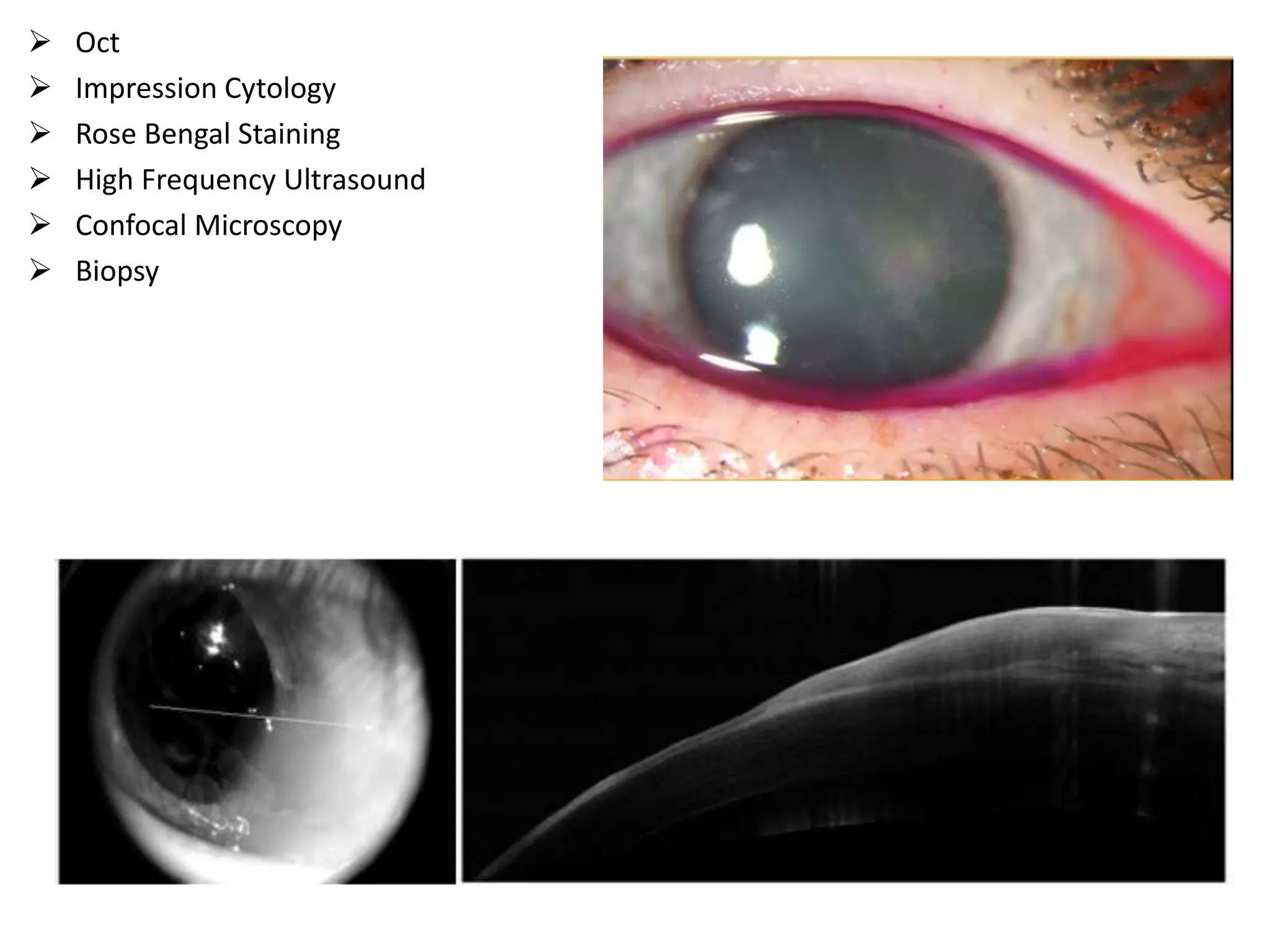
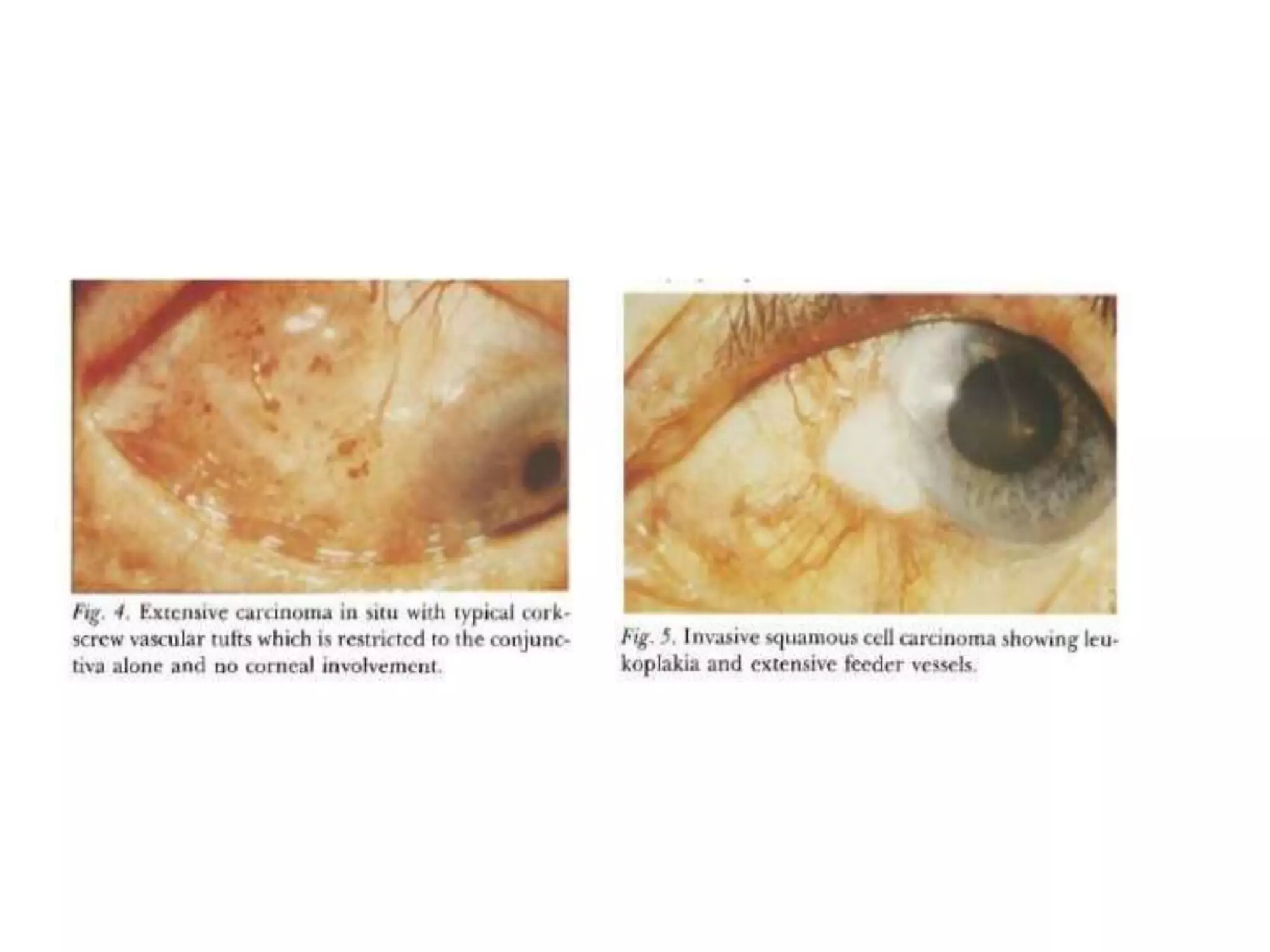
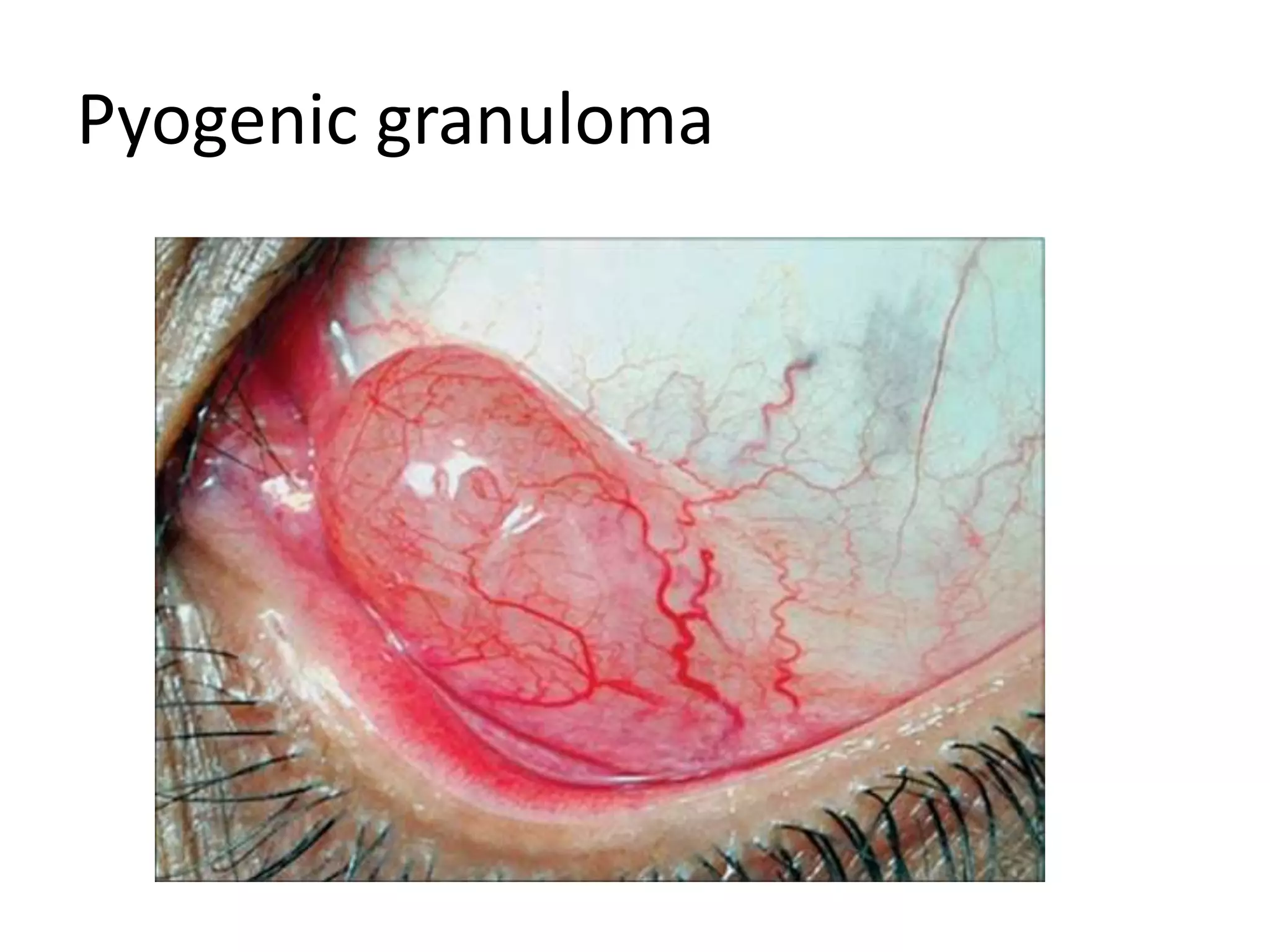
- Diagnosis is usually based on appearance of a red, elevated mass with intrinsic vessels or feeder vessels. Advanced cases can infiltrate the cornea, sclera, or orbit.
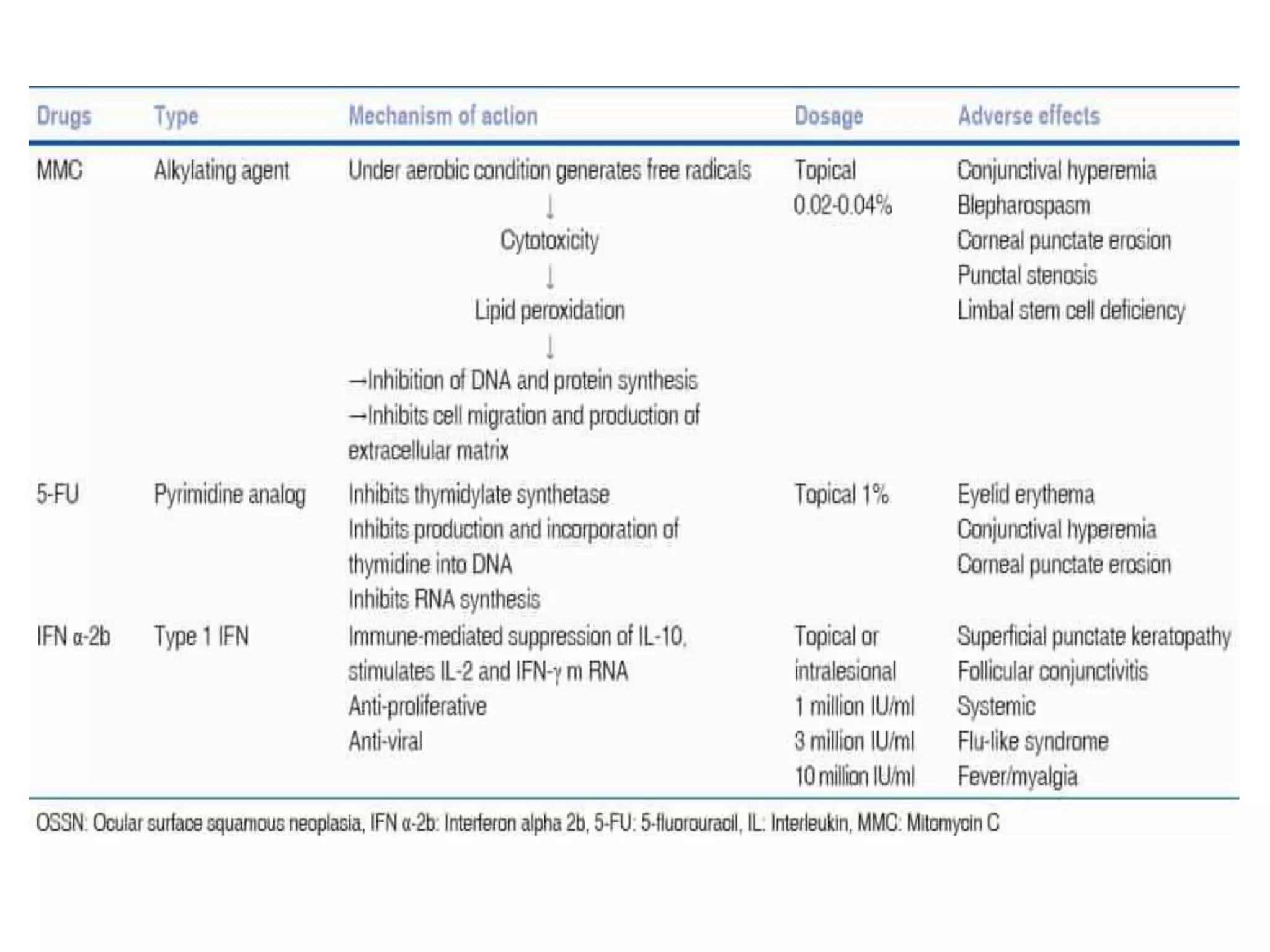
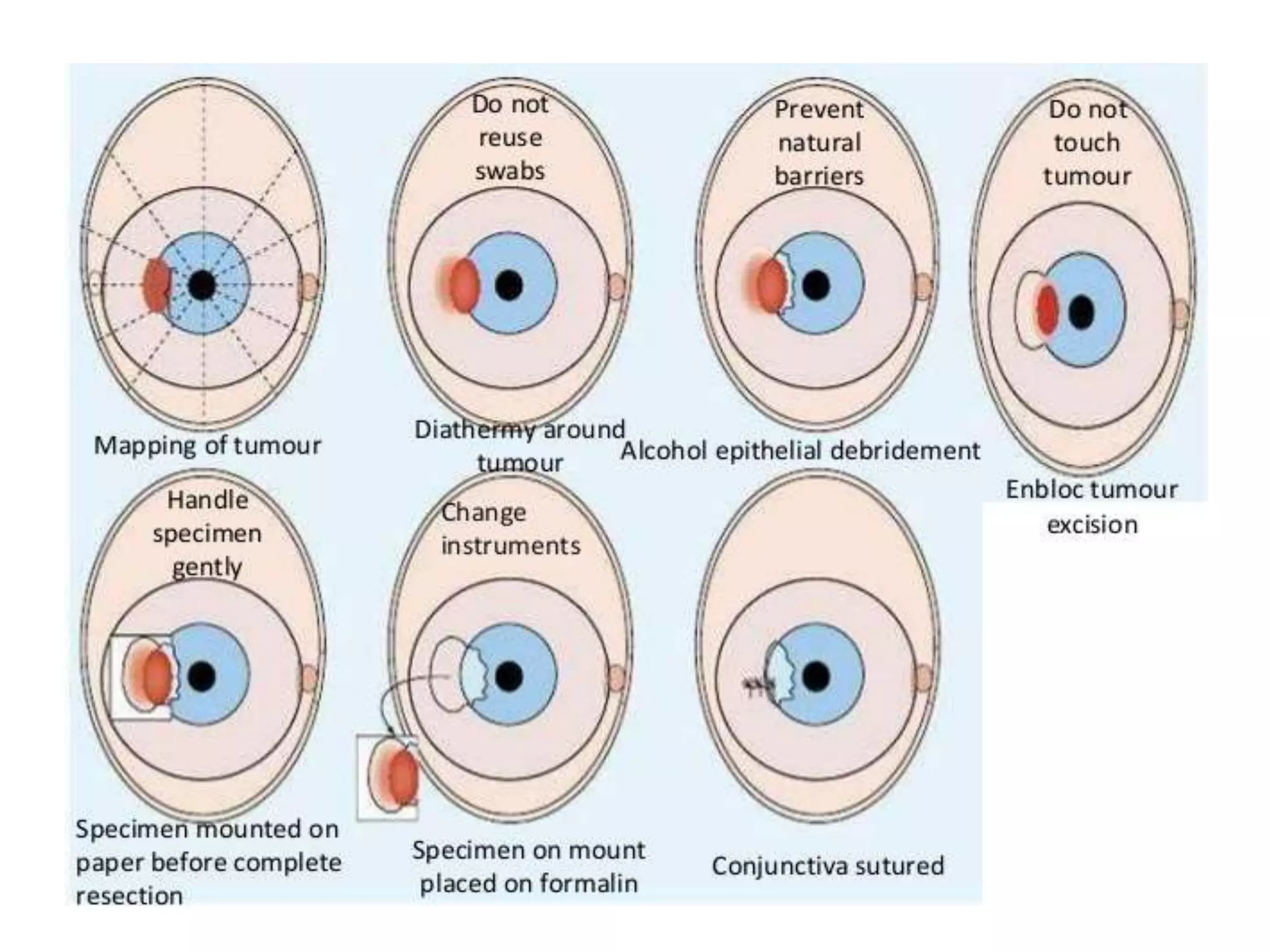
- Treatment involves surgical excision with clear margins followed by cryotherapy. Recurrence rates after surgery are over 50%