Downloaded 30 times


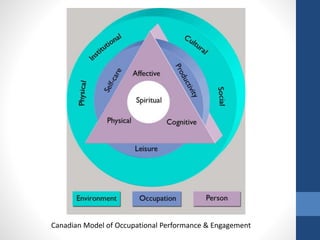
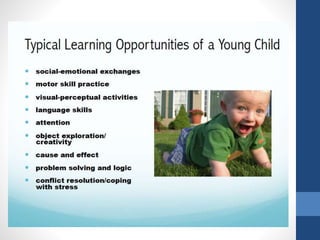
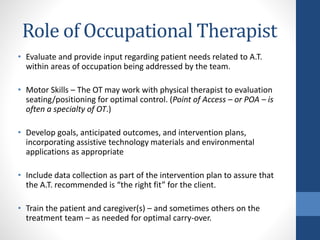



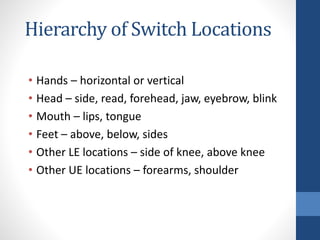

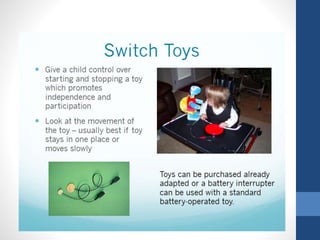

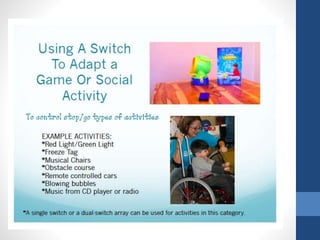
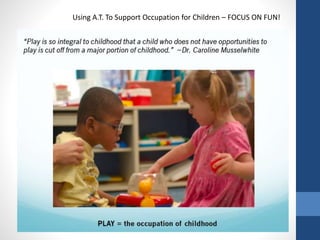

The document discusses the role of occupational therapists in assistive technology. It describes how occupational therapists can evaluate patients' needs related to areas like motor skills, communication, mobility, and cognition to determine what assistive technologies could help. Occupational therapists then develop goals and intervention plans incorporating appropriate assistive technologies. They train patients and caregivers on proper use of assistive technologies to ensure optimal outcomes. The document provides examples of how occupational therapists evaluate seating and positioning needs, as well as types of switches that can be used based on different body locations. It emphasizes that occupational therapists focus on fun when using assistive technology to support children's occupations.