Downloaded 66 times



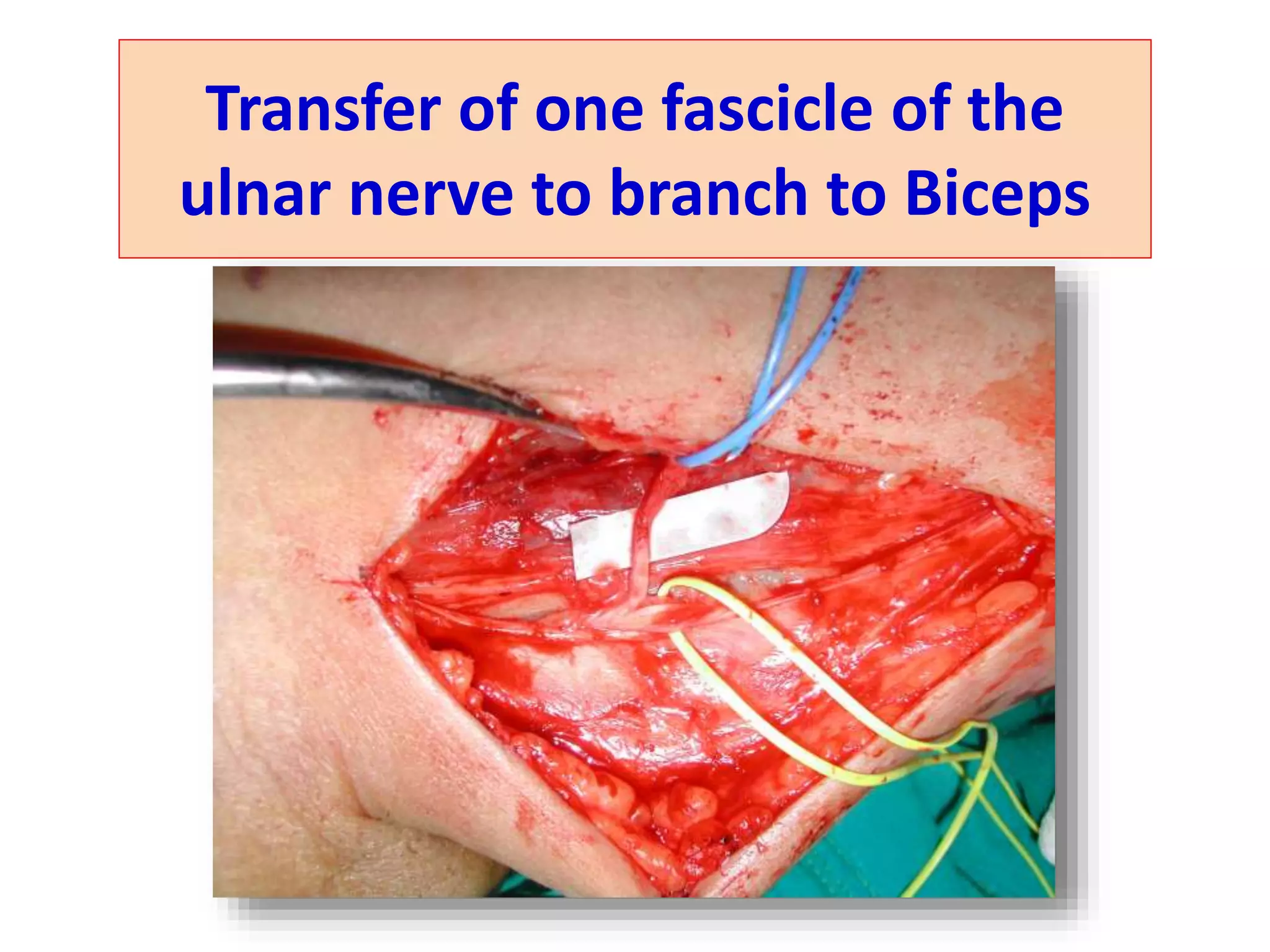


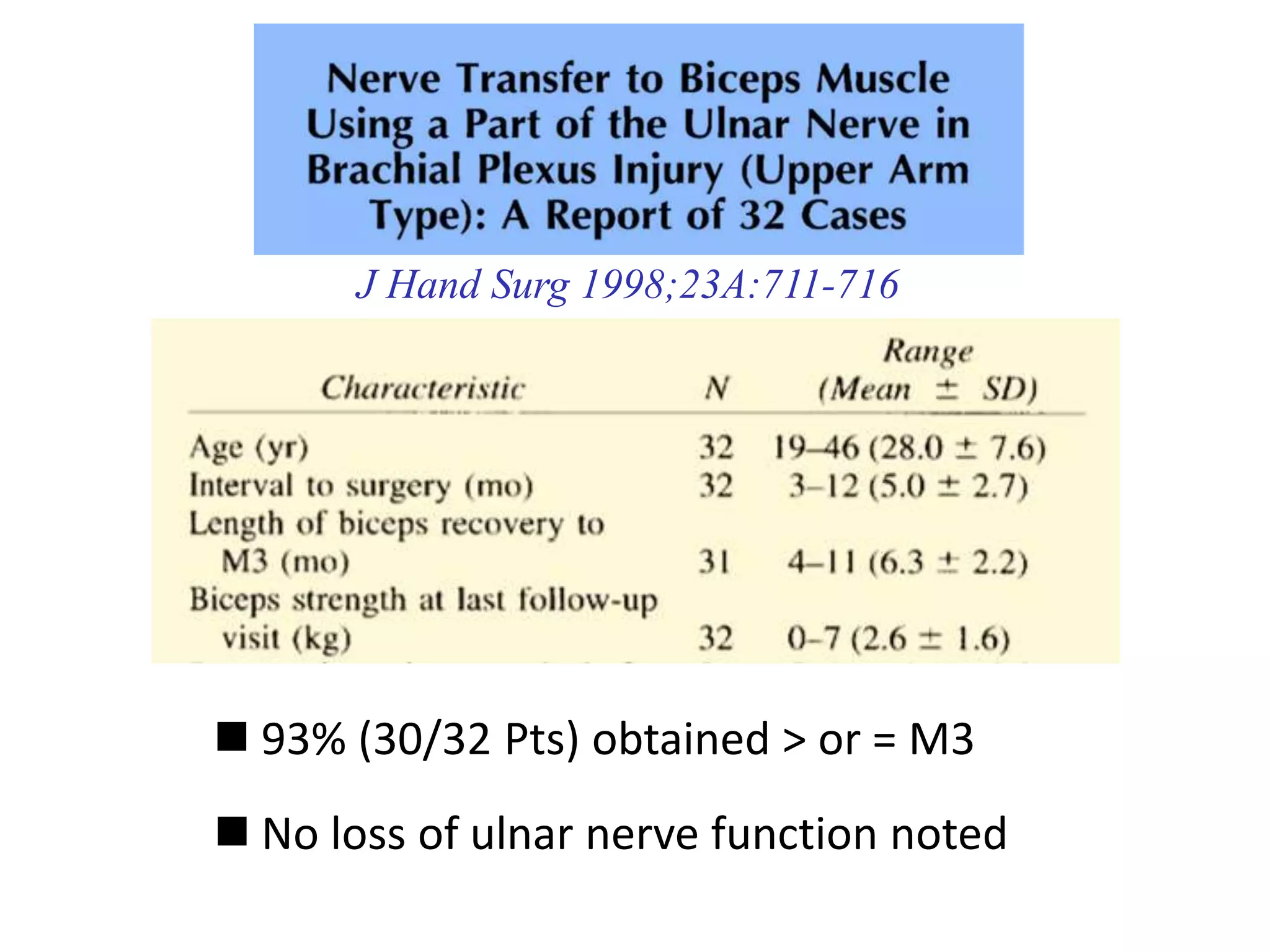






This document discusses two Oberlin nerve transfer techniques for restoring elbow flexion after brachial plexus injury: 1. Oberlin I involves transferring a fascicle of the ulnar nerve to the motor branch of the biceps muscle. Over 100 patients who underwent this procedure regained M3 or greater elbow flexion strength, with recovery occurring between 5-11 months. 2. Oberlin II adds transferring a fascicle of the median nerve to the motor branch of the brachialis muscle. This "dual nerve transfer" technique was illustrated in a patient who showed recovery of both the biceps and brachialis muscles 10 months post-operatively. The Oberlin techniques rely on the proximity























































































