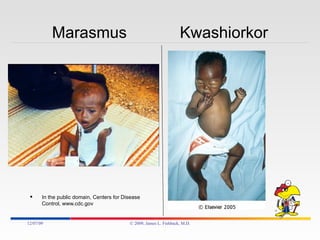
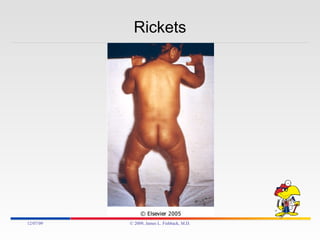
The document discusses various nutritional deficiencies and toxicities that can threaten human health, including protein-energy malnutrition, vitamin deficiencies, and mineral deficiencies. It provides details on specific deficiencies such as scurvy (vitamin C deficiency), beriberi (thiamine deficiency), rickets (vitamin D deficiency), and anemia (iron deficiency). It also covers protein-energy malnutrition conditions like marasmus, kwashiorkor, and secondary protein-energy malnutrition.
































![[3] Nutritional Disorders (Combined)](https://cdn.slidesharecdn.com/ss_thumbnails/3nutritionaldisorderscombined-091208012618-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


![VITAMIN K, [MEDICINAL CHEMISTRY] BY P.RAVISANKAR,STRUCTURES OF VITAMIN K1 AND...](https://cdn.slidesharecdn.com/ss_thumbnails/phm10vitk-130615194322-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












