
Download as PDF, PPTX



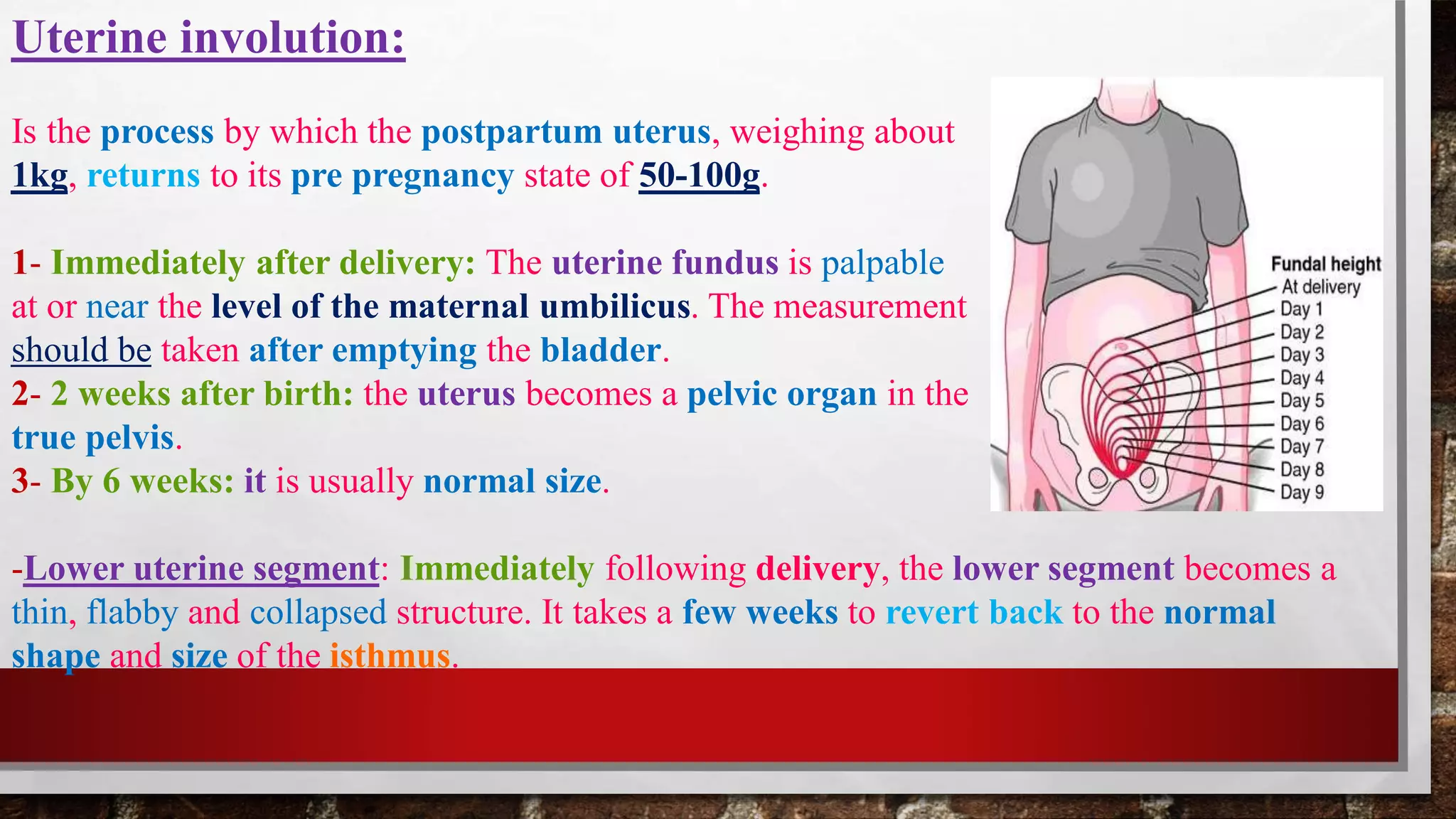


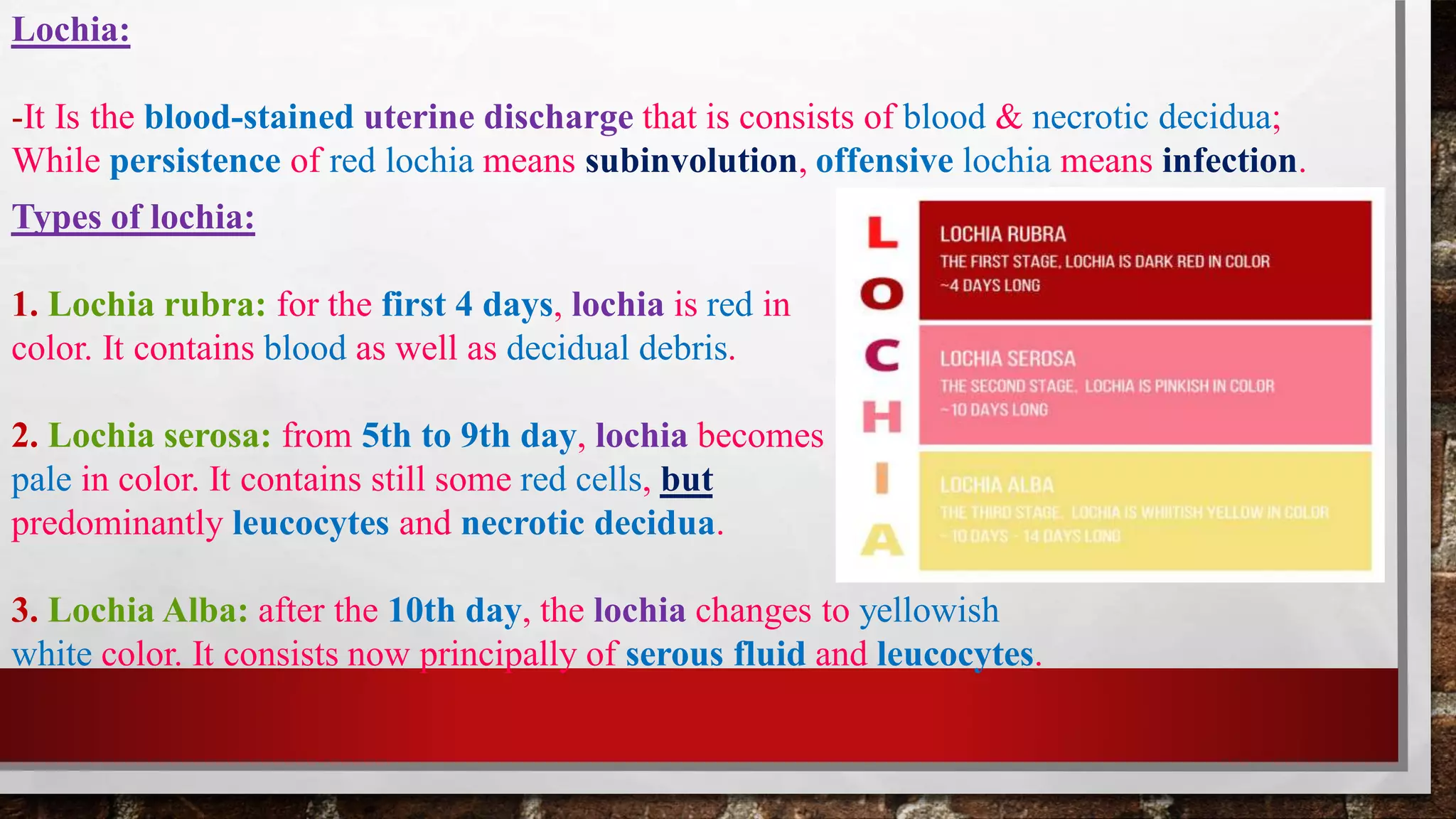




















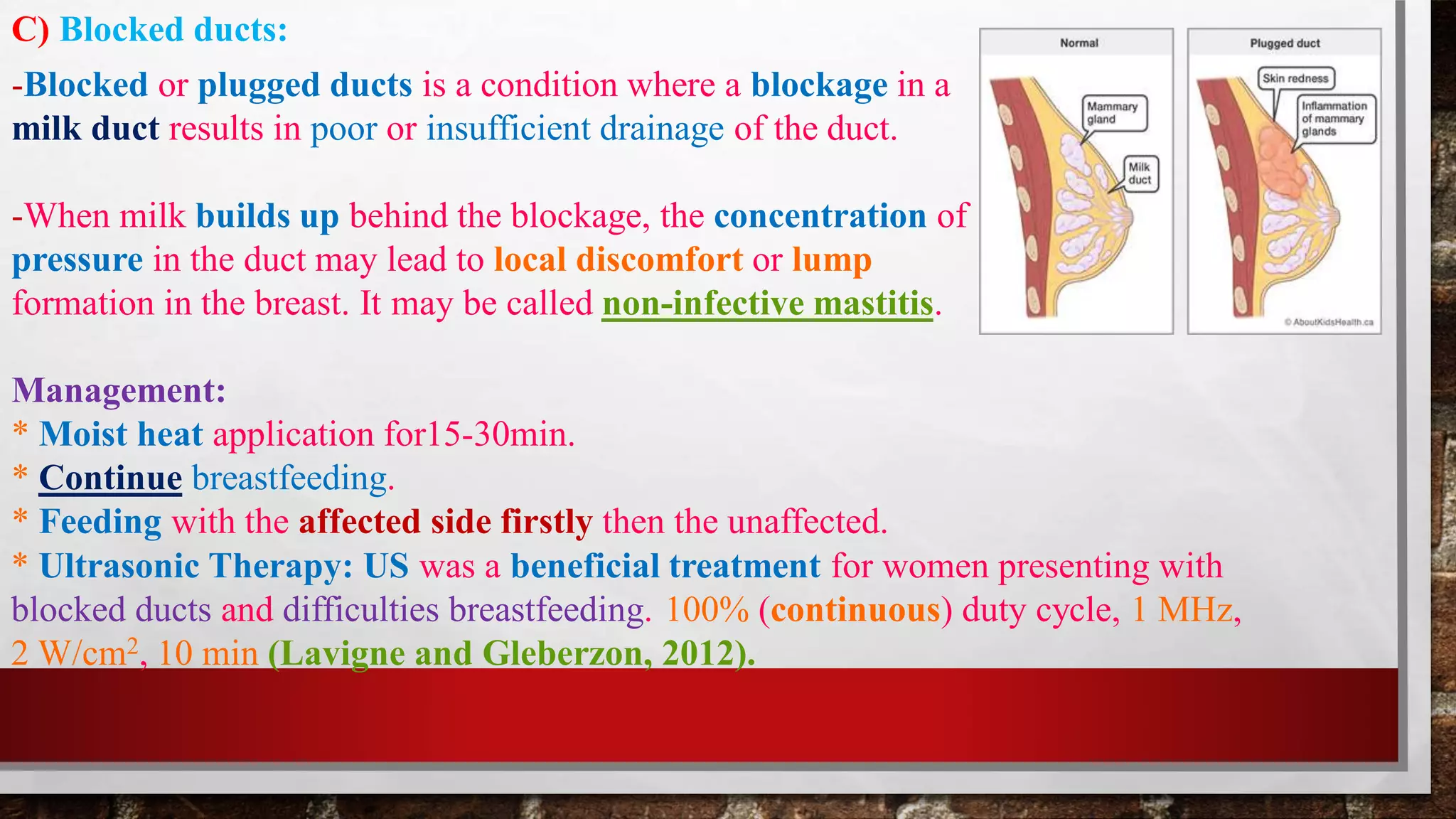
















- Puerperium refers to the 6-week period following delivery where the body returns to its pre-pregnant state. This involves involution of the uterus, breasts, and other organs as well as hormonal and physiological changes. - Common issues during this period include uterine and breast involution, lochia, urinary changes, weight loss, endocrine changes, and psychological adjustment. Complications can include postpartum hemorrhage, infection, retained placenta, and painful perineum. Physical therapy modalities like cryotherapy, TENS, LLLT, and pelvic floor exercises can help manage pain.






















































































