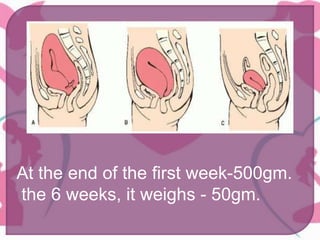
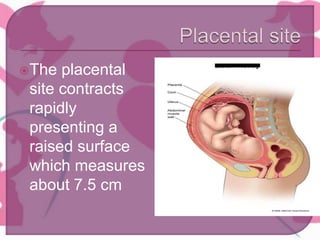
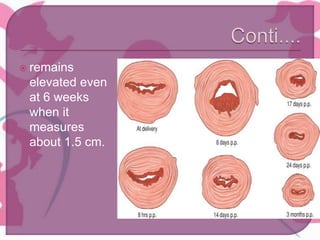
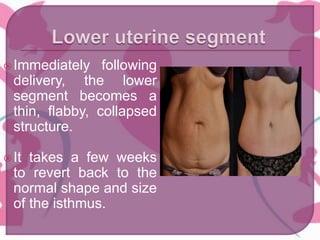
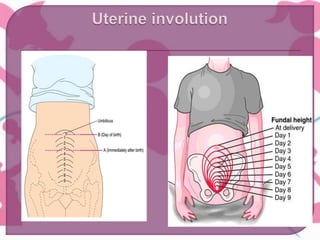
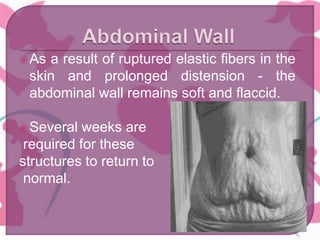
The document summarizes physiological changes that occur during the postpartum period known as the puerperium. It lasts approximately 6 weeks as the body reverts back to its pre-pregnant state. This includes involution of the uterus, vagina, and other pelvic structures. Other changes include lochia discharge, temperature regulation returning to normal, changes in blood pressure and pulse, weight loss, fluid balance changes, and the return of menstruation being delayed in women who breastfeed.


















































![Normal_Puerperium [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/normalpuerperium1-241127062853-ff043941-thumbnail.jpg?width=640&height=640&fit=bounds)



















