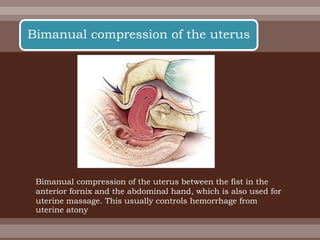
The document discusses postpartum care and complications. It covers the anatomical changes that occur after delivery, routine postpartum care including monitoring for bleeding and infection, complications like postpartum hemorrhage, and patient education on caring for themselves and their newborn. Discharge instructions advise women on resuming normal activities and making follow-up appointments.



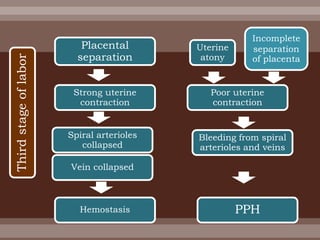
![ Objectively, postpartum hemorrhage is
defined as a 10% change in hematocrit level
between admission and the postpartum
period or the need for transfusion after
delivery secondary to blood loss.[3 ]
10% change in hematocrit
Postpartum hemorrhage
(continue)](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-57-320.jpg)
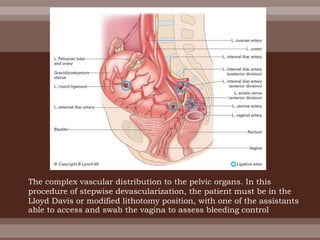
![ When conservative therapy fails, the next step is
surgery with either bilateral uterine artery ligation or
hypogastric artery ligation.
Uterine artery ligation is thought to be successful in
80-95% of patients.
If this therapy fails, hypogastric artery ligation is an
option. However, this approach is technically difficult
and is only successful in 42-50% of patients.[14 ]](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-96-320.jpg)
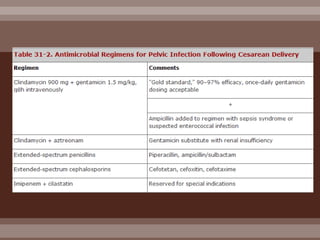
![ This combination is not effective against Enterococcus
faecalis, which may be the cause in up to 25% of
these infections.
The addition of ampicillin (or vancomycin for patients
with a penicillin allergy), is considered when the
patient does not respond to the initial therapy of
gentamicin and clindamycin to cover this organism. ]
Ampicillin
Vancomycin
Enterococcus faecalis](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-130-320.jpg)
![ The timing of prophylaxis is also an issue; 2 recent
studies showed lower rates of infection when
antimicrobial prophylaxis occurred before skin
incision vs after cord clamping.[27,28
]However, another trial that studied the same timing
issue found that the timing of prophylaxis did not
affect maternal infectious morbidity.[29 ]](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-135-320.jpg)



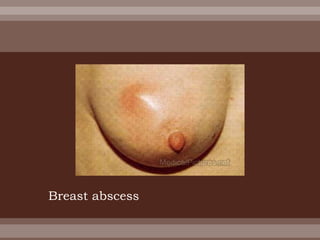
![ The most common causative organism,
isolated in approximately half of all cases, is
Staphylococcus aureus.[32 ]
Other common pathogens include
Staphylococcus epidermidis, S saprophyticus,
Streptococcus viridans, and E coli.](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-161-320.jpg)
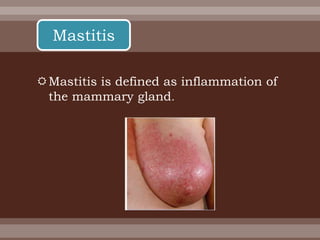
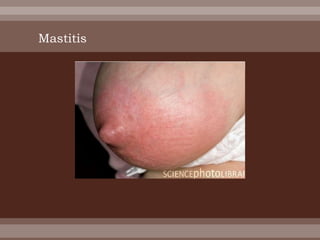
![ In the United States, the incidence of
postpartum mastitis is 2.5-3%.[33,32 ]
Mastitis typically develops during the first 3
months postpartum, with the highest
incidence in the first few weeks after
delivery.
Incidence](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-162-320.jpg)



![ : Abdominal wound infections are most frequently the
result of contamination with vaginal flora.
However, S aureus, either from the skin or from an
exogenous source, is isolated in 25% of these
infections.[34 ]
Genital Mycoplasma species are commonly isolated
from infected wounds that are resistant to treatment
with penicillins.[35 ]
Abdominal wound infections](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-185-320.jpg)

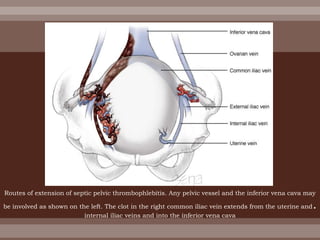
![ Septic pelvic thrombophlebitis occurs in 1 of every
2000-3000 pregnancies and is
10 times more common after cesarean birth (1 per
800) than after vaginal delivery (1 per 9000).[38 ]
The condition affects less than 1% of patients with
endometritis.
Incidence](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-206-320.jpg)
![ Initially, it was thought that patients defervesce
within 24-28 hours.[40 ]More recent studies show that
it takes 5-6 days for the fevers to resolve.[40,41 ]](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-217-320.jpg)
![ In a 1999 prospective randomized study, women who
were treated with heparin in addition to antibiotics
responded no faster than patients treated with
antibiotics alone.[38 ]
These findings do not support the empiric practice of
heparin therapy for septic pelvic thrombophlebitis
and raise the question of whether a new standard
protocol should be developed](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-218-320.jpg)
![ Prevalence and Types Postpartum thyroid
dysfunction can occur any time in the first
postpartum year.
Clinical or laboratory dysfunction occurs in 5-10% of
postpartum women and may be caused by primary
disorders of the thyroid, such as postpartum
thyroiditis (PPT) and Graves disease, or by secondary
disorders of the hypothalamic-pituitary axis, such as
Sheehan syndrome and lymphocytic hypophysitis.[42 ]
Endocrine Disorders](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-220-320.jpg)
![ The first laboratory test to be performed should be
the thyroid-stimulating hormone (TSH) test.[44 ]
TSH is decreased during the thyrotoxicosis stage and
increased during the hypothyroid phase
If the TSH level is abnormal, check thyroid
stimulating antibodies, free thyroxine index (FTI), and
radioactive iodine uptake (RIU) in order to distinguish
this disorder from Graves disease.
Workup](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-227-320.jpg)
![ In PPT, RIU is low, thyroid-stimulating antibodies are
undetectable, and FTI is high.
Thorough, cost-effective screening test for PPT does
not exist; therefore, limit screening to high-risk
patients such as those with previous PPT or other
autoimmune disorders.[45 ]](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-228-320.jpg)
![No treatment is available to prevent
PPT.[45 ]
Treatment](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-229-320.jpg)
![ Approximately 50-70% of women who have given
birth develop symptoms of postpartum blues.
PPD occurs in 10-15% of new mothers.[46 ]
The incidence of postpartum or puerperal psychosis
is 0.14-0.26%.
Incidence](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-249-320.jpg)
![ Psychiatric disorders can have deleterious
effects on the social, cognitive, and
emotional development of the newborn.[47
]These ailments can also lead to marital
difficulties.
Morbidity and mortality](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-250-320.jpg)
![ Definition of puerperal fever
A temperature rise above 100.0 °F (38°C) maintained
over 24 hours or recurring during the period from the
end of the first to the end of the 10th day after
childbirth or abortion. (ICD-10)
Oral temperature of 100.0 °F (38°C) or more on any
two of the first ten days postpartum. (USJCMW)[6]](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-262-320.jpg)
![ Terminology
Puerperal fever is no longer favored as a diagnostic category.
Instead, contemporary terminology specifies:[1]
the specific target of infection: endometritis (inflammation of
the inner lining of the uterus), metrophlebitis (inflammation of
the veins of the uterus), and peritonitis (inflammation of the
membrane lining of the abdomen)
the severity of the infection: (relatively) uncomplicated infection
(contained multiplication of microbes), and possibly life-
threatening sepsis (uncontrolled and uncontained
multiplication of microbes throughout the blood stream).](https://image.slidesharecdn.com/rholztrdqryls9lplccf-signature-81d8d6183cc46b90d3861bdee3e9c1d01243057be108a550b2d453be1d558f89-poli-150321225613-conversion-gate01/85/020-normal-and-abnormal-puerperium-2-263-320.jpg)