
Download as PDF, PPTX


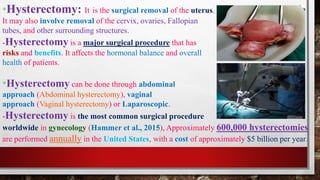

Hysterectomy is a surgical procedure to remove the uterus, and sometimes other female reproductive organs. It is one of the most common gynecological surgeries, with over 600,000 performed annually in the US. There are several types of hysterectomy that are performed depending on factors like the surgical approach and extent of organ removal. Physical therapy both before and after hysterectomy aims to improve patient strength, mobility, and recovery through exercises targeting the core, pelvic floor, breathing, and circulation. Complications can include infection, incontinence, and prolapse, so physical therapy also focuses on preventing and managing these issues.













































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)





