Steel toe capped boots are commonly worn for foot protection in industrial settings. However, there is little data on how steel toes affect injury patterns. This study examined crush injuries to cadaver feet with and without steel toes, finding that steel toes reduced the number and severity of fractures compared to regular boots, but did not fully prevent injury.
In this article, we present the general principle of management Periprosthetic fracture after arthroplasty according to the "Unified” or “Comprehensive” classification system. We especially review the current concepts of periprosthetic hip and knee fractures.
Corrective Surgery for Malunited Tibial Plateau Fractureiosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
Management of atypical THA periprosthetic fracture RiverTsai2
There increasing cases of atypical THA periprosthetic fracture after long term anti-osteoporosis agent use,especially biphosphonates. It has special characteristics form traditional Vancouver periprosthetic fracture. The speech is delivered by Dr. Chun-Hao Tsai of China Medical University Hospital ,Taichung,Taiwan.
This journal club presents a case of prosthetic
rehabilitation of an amputated thumb. It emphasizes that
prosthetic replacement is a better option for aesthetic and
psychological improvement, particularly in cases where the
victim is unwilling to undergo complicated surgical procedures for reconstruction of thumb or where functioning
of thumb cannot be restored even by multiple surgeries. In
the present case, a 20 years old female patient, with
missing thumb of her right hand was rehabilitated aesthetically by a non-invasive and cost effective prosthetic
procedure by using heat temperature vulcanizing silicone
material. The prosthesis (the thumb) was attached using
medical adhesives. On 3 months recall appointment, no
complications were observed. The prosthesis was in good
shape and required no further intervention. The prosthetic
thumb lacks the sensation of a normal or reconstructed
thumb, although it does not require the multiple procedures
of surgical reconstruction and the accompanying loss of
time for rehabilitation and healing
In this article, we present the general principle of management Periprosthetic fracture after arthroplasty according to the "Unified” or “Comprehensive” classification system. We especially review the current concepts of periprosthetic hip and knee fractures.
Corrective Surgery for Malunited Tibial Plateau Fractureiosrjce
IOSR Journal of Dental and Medical Sciences is one of the speciality Journal in Dental Science and Medical Science published by International Organization of Scientific Research (IOSR). The Journal publishes papers of the highest scientific merit and widest possible scope work in all areas related to medical and dental science. The Journal welcome review articles, leading medical and clinical research articles, technical notes, case reports and others.
Management of atypical THA periprosthetic fracture RiverTsai2
There increasing cases of atypical THA periprosthetic fracture after long term anti-osteoporosis agent use,especially biphosphonates. It has special characteristics form traditional Vancouver periprosthetic fracture. The speech is delivered by Dr. Chun-Hao Tsai of China Medical University Hospital ,Taichung,Taiwan.
This journal club presents a case of prosthetic
rehabilitation of an amputated thumb. It emphasizes that
prosthetic replacement is a better option for aesthetic and
psychological improvement, particularly in cases where the
victim is unwilling to undergo complicated surgical procedures for reconstruction of thumb or where functioning
of thumb cannot be restored even by multiple surgeries. In
the present case, a 20 years old female patient, with
missing thumb of her right hand was rehabilitated aesthetically by a non-invasive and cost effective prosthetic
procedure by using heat temperature vulcanizing silicone
material. The prosthesis (the thumb) was attached using
medical adhesives. On 3 months recall appointment, no
complications were observed. The prosthesis was in good
shape and required no further intervention. The prosthetic
thumb lacks the sensation of a normal or reconstructed
thumb, although it does not require the multiple procedures
of surgical reconstruction and the accompanying loss of
time for rehabilitation and healing
Stress & force factors in implants /certified fixed orthodontic courses by I...Indian dental academy
The Indian Dental Academy is the Leader in continuing dental education , training dentists in all aspects of dentistry and offering a wide range of dental certified courses in different formats.
Indian dental academy provides dental crown & Bridge,rotary endodontics,fixed orthodontics,
Dental implants courses.for details pls visit www.indiandentalacademy.com ,or call
0091-9248678078
This paper of finite element analysis of the rib cage model is applied to recognize stress distributions and to determine the rate of bone fractures(especially for pathologically changed bones). Also to determine the load and stress to occurs on the human rib cage at any accident. Also find the maximum load sustain capacity of human rib cage and according to the load sustain capacity of the human rib cage by finite element analysis and search a material as like a bone cement and it take on a rib fracture and see the result . This paper is only of to nullify the rib fracture as present medical treatment give the elastic belt but due to respiration, the human ribs are contract and relax that’s the rib fracture are only minimize not a nullify. The human models are considered in between age 15 to 40 year. The Simulation result shows a good agreement with the cadaver test data.
Slides from Prof Dan Pratt presented at the Teaching to Teach Workshop in Boston, MA, May 1-2, 2009;
Massachusetts General Hospital, Harvard Medical School.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
The hemodynamic and autonomic determinants of elevated blood pressure in obes...
Crush Injuries to the Forefoot
1. P A R T N E R S O R T H O P A E D I C
Trauma Rounds
Case Reports from the Mass General Hospital and Brigham & Women’s Hospital
A Quarterly Case Study Volume 3, Spring 2012
Crush Injuries to the Forefoot
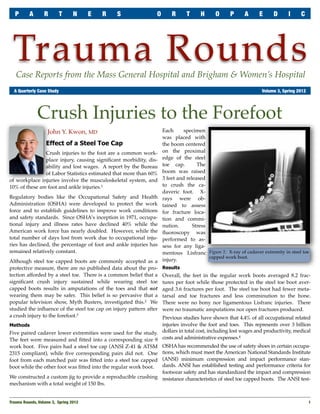
John Y. Kwon, MD Each specimen
was placed with
Effect of a Steel Toe Cap the boom centered
Crush injuries to the foot are a common work- on the proximal
place injury, causing significant morbidity, dis- edge of the steel
ability and lost wages. A report by the Bureau toe cap. The
of Labor Statistics estimated that more than 60% boom was raised
of workplace injuries involve the musculoskeletal system, and 3 feet and released
10% of these are foot and ankle injuries.1 to crush the ca-
daveric foot. X-
Regulatory bodies like the Occupational Safety and Health rays were ob-
Administration (OSHA) were developed to protect the work tained to assess
force and to establish guidelines to improve work conditions for fracture loca-
and safety standards. Since OSHA’s inception in 1971, occupa- tion and commi-
tional injury and illness rates have declined 40% while the nution. Stress
American work force has nearly doubled. However, while the fluoroscopy was
total number of days lost from work due to occupational inju- performed to as-
ries has declined, the percentage of foot and ankle injuries has sess for any liga-
remained relatively constant. mentous Lisfranc Figure 1: X-ray of cadaver extremity in steel toe
capped work boot.
Although steel toe capped boots are commonly accepted as a injury.
protective measure, there are no published data about the pro- Results
tection afforded by a steel toe. There is a common belief that a Overall, the feet in the regular work boots averaged 8.2 frac-
significant crush injury sustained while wearing steel toe tures per foot while those protected in the steel toe boot aver-
capped boots results in amputations of the toes and that not aged 3.6 fractures per foot. The steel toe boot had fewer meta-
wearing them may be safer. This belief is so pervasive that a tarsal and toe fractures and less comminution to the bone.
popular television show, Myth Busters, investigated this.2 We There were no bony nor ligamentous Lisfranc injuries. There
studied the influence of the steel toe cap on injury pattern after were no traumatic amputations nor open fractures produced.
a crush injury to the forefoot.3 Previous studies have shown that 4.4% of all occupational related
Methods injuries involve the foot and toes. This represents over 3 billion
Five paired cadaver lower extremities were used for the study. dollars in total cost, including lost wages and productivity, medical
The feet were measured and fitted into a corresponding size 9 costs and administrative expenses.
4
work boot. Five pairs had a steel toe cap (ANSI Z-41 & ATSM OSHA has recommended the use of safety shoes in certain occupa-
2315 compliant), while five corresponding pairs did not. One tions, which must meet the American National Standards Institute
foot from each matched pair was fitted into a steel toe capped (ANSI) minimum compression and impact performance stan-
boot while the other foot was fitted into the regular work boot. dards. ANSI has established testing and performance criteria for
footwear safety and has standardized the impact and compression
We constructed a custom jig to provide a reproducible crushing resistance characteristics of steel toe capped boots. The ANSI test-
mechanism with a total weight of 150 lbs.
Trauma Rounds, Volume 3, Spring 2012
1
2. P A R T N E R S O R T H O P A E D I C T R A U M A R O U N D S
the ANSI protocol we found no toe amputations nor complete
failures of the steel toe cap.
Although steel toe capped boots are commonly accepted as a pro-
tective measure, there are no published data about how protection
afforded by a steel toe influences foot fracture epidemiology. This
study demonstrated that the steel toe protects the foot from crush
injuries, limiting the number and severity of forefoot fractures.
However, the steel toe cap does not fully protect the forefoot from
injury and in addition to the use of safety shoes, strict adherence to
workplace safety standards may limit the severity of crush injuries
to the foot.
Acknowledgements
I would like to acknowledge my fellow myth busters: John T.
Figure 2: X-ray of a cadaveric forefoot after crush impact in a regular
work boot (left) and in a steel toe capped work boot (right). Campbell, MD, Mark S. Myerson, MD and Cliff L. Jeng, MD.
Dr. John Kwon (Jkwon@partners.org) is an orthopaedic surgeon at the Massa-
ing consists of a steel weight weighing 50 lbs (±0.5 lbs) dropped chusetts General Hospital, Boston and a member of the Foot & Ankle Service, as
from a height of 3 feet. 5, 6 well as the Partners Orthopaedic Trauma Service. Dr. Kwon specializes in foot
& ankle fractures, sports injuries and correction of foot & ankle deformities.
Conclusions
Bibliography
In our study we tripled this weight to ensure the creation of frac- 1. Bureau of Labor Statistics. Care and demographic characteristics for work-related
tures in our non-protected specimens and to elucidate the protec- injury and illness involving days away from work. Washington, DC: Bureau of
tive nature of the steel cap. Even when tripling the weight used by Labor Statistics, US Department of Labor; 1992 – 1999.
2. MythBusters, Episode 42, Discovery Channel: November 9, 2005
3. Kwon JY, Campbell JT, Myerson MS, Jeng CL, Effect of a steel toe cap on forefoot
injury pattern in a cadaveric model. Foot and Ankle Int. 2011 Apr; 32(4):443-7.
4. Campbell, JT: Foot and ankle fractures in the industrial setting. Foot Ankle Clin.
7(2):323 – 50, 2002.
5. Bureau of Labor Statistics. Labor force statistics from the current population sur-
vey. Washington, DC: Bureau of Labor Statistics. US Department of Labor;
2001.
6. Bureau of Labor Statistics. Lost worktime injuries and illnesses: characteristics
and resulting time away from work, 1999. Washington, DC: Bureau of Labor
Statistics, US Department of Labor; 1999.
In Memoriam
Figure 3: Steel toe cap after crush impact (left) compared to an
uncrushed steel toe cap (right). Edward "Teddy" Kim
September 3, 1984 - April 6, 2012
We are saddened to report the passing of our friend and former col-
league, Teddy Kim, who recently passed away after a yearlong battle
AchesAndJoints.org/Trauma with leukemia. Teddy worked with us as a research assistant during his
junior and senior years at Boston College. He will be missed.
Jesse Jupiter, MD — 617-726-5100 Please share your comments online, or by email:
Trauma Faculty MGH Hand & Upper Extremity Service Mark Vrahas, MD / mvrahas@partners.org
Mark Vrahas, MD — 617-726-2943 jjupiter@partners.org Yawkey Center for Outpatient Care, Suite 3C
Partners Chief of Orthopaedic Trauma 55 Fruit Street, Boston, MA 02114
mvrahas@partners.org David Ring, MD — 617-724-3953
Mitchel B Harris, MD — 617-732-5385
MGH Hand & Upper Extremity Service Editor in Chief
dring@partners.org
Chief, BWH Orthopedic Trauma Mark Vrahas, MD
mbharris@partners.org Brandon E Earp, MD — 617-732-8064
R Malcolm Smith, MD, FRCS — 617-726-2794 BWH Hand & Upper Extremity Service Program Director
bearp@partners.org
Chief, MGH Orthopaedic Trauma Suzanne Morrison, MPH
rmsmith1@partners.org George Dyer, MD — 617-732-6607 (617) 525-8876
BWH Hand & Upper Extremity Service smmorrison@partners.org
David Lhowe, MD — 617-724-2800
MGH Orthopaedic Trauma gdyer@partners.org
dlhowe@partners.org
Editor, Publisher
John Kwon, MD — 617-643-5701 Arun Shanbhag, PhD, MBA
Michael Weaver, MD — 617-525-8088 MGH Foot & Ankle Service
BWH Orthopedic Trauma www.MassGeneral.org/ortho
jkwon@partners.org
mjweaver@partners.org www.BrighamAndWomens.org/orthopedics
2
Trauma Rounds, Volume 3, Spring 2012