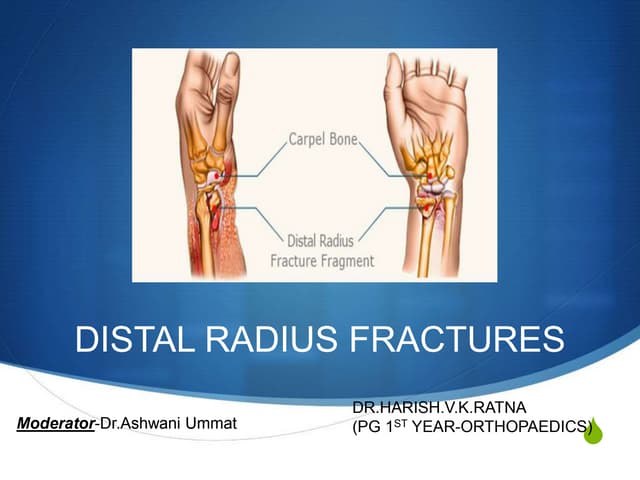
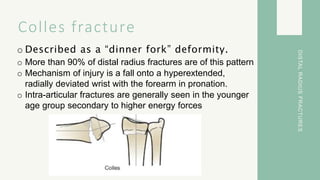
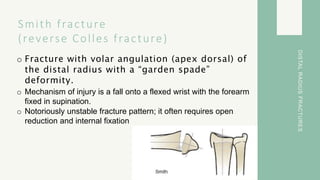
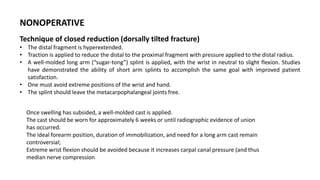
This document summarizes different types of distal radius fractures, including Colles fractures and Smith fractures. Colles fractures involve a hyperextended and radially deviated wrist from a fall, often appearing as a "dinner fork" deformity. Smith fractures are the reverse with volar angulation from the wrist flexed in a fall. Treatment options are also summarized, indicating nonoperative treatment for nondisplaced or minimally displaced fractures using splinting or casting, while operative indications include displaced articular fractures, nerve injuries, or multiple injuries. Nonoperative techniques involve closed reduction and splinting or casting the wrist in slight flexion for 6 weeks.















![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)