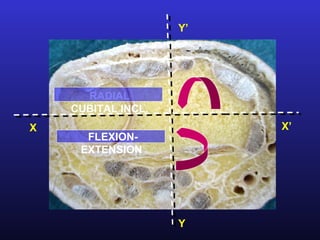
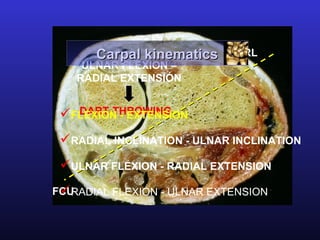
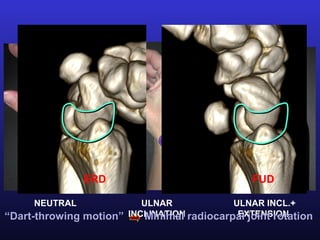
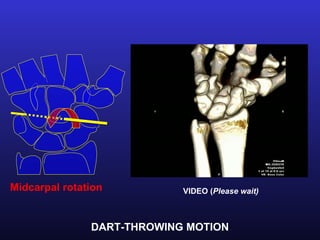
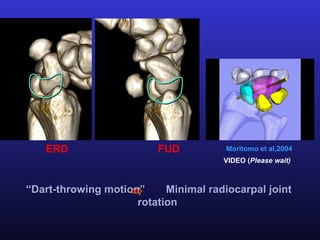
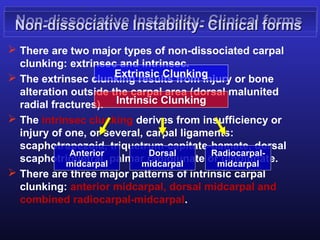
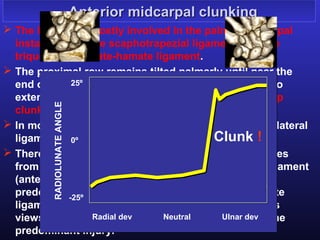
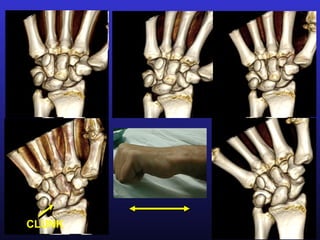
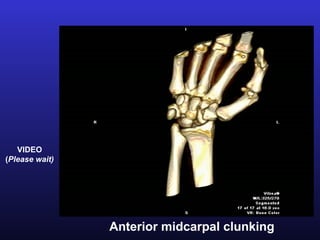
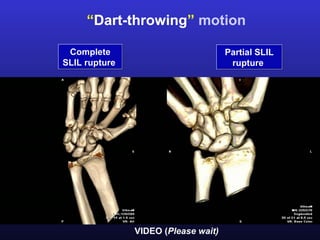
Four-dimensional CT can be used to evaluate dynamic wrist instabilities. It allows visualization of carpal kinematics during various wrist motions like flexion-extension and dart throwing. This helps characterize patterns of non-dissociative carpal clunking and differentiate partial from complete tears of the scapholunate ligament, improving diagnosis of wrist instability types.