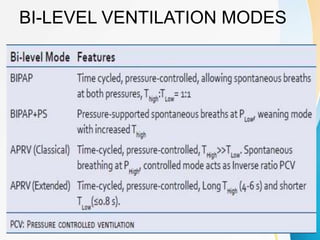
The document discusses several newer modes of mechanical ventilation that aim to improve patient-ventilator synchrony and reduce ventilator-induced lung injury compared to traditional open-loop modes. These include modes that provide dual control within or between breaths, target a minimum tidal volume, proportionally assist patient effort, and use the diaphragm's electrical activity to synchronize ventilation. The document also describes a "smart" closed-loop mode that aims to mimic clinical weaning protocols.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






