Download to read offline




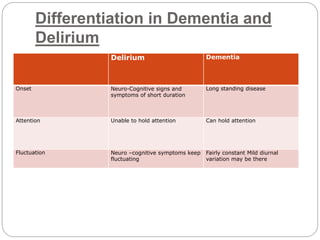
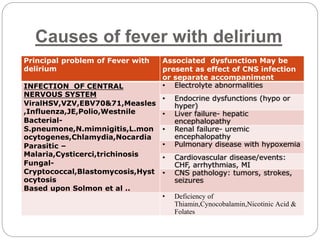

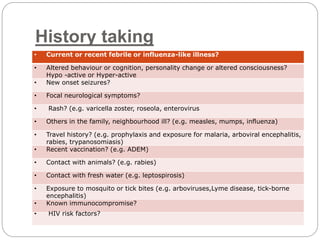












The document presents a comprehensive overview of fever with delirium, highlighting its definition, clinical characteristics, types, etiology, risk factors, and management strategies. It emphasizes the high incidence and mortality rates, particularly in children, and discusses the multifactorial causes as well as the importance of differentiating delirium from dementia. The document concludes with treatment recommendations and the need for supportive care, rehabilitation, and effective antibiotic therapy.


















































































