Downloaded 39 times







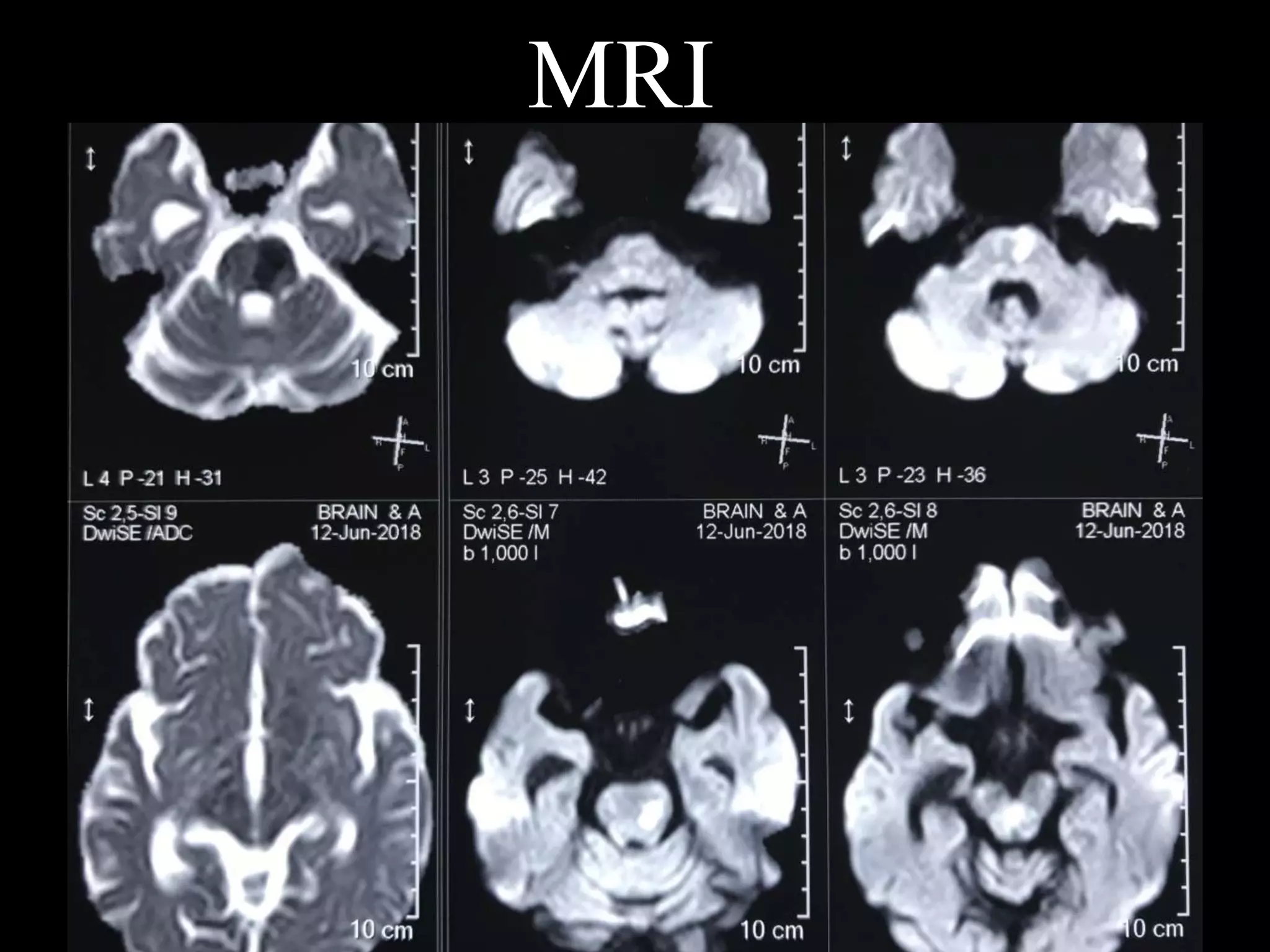


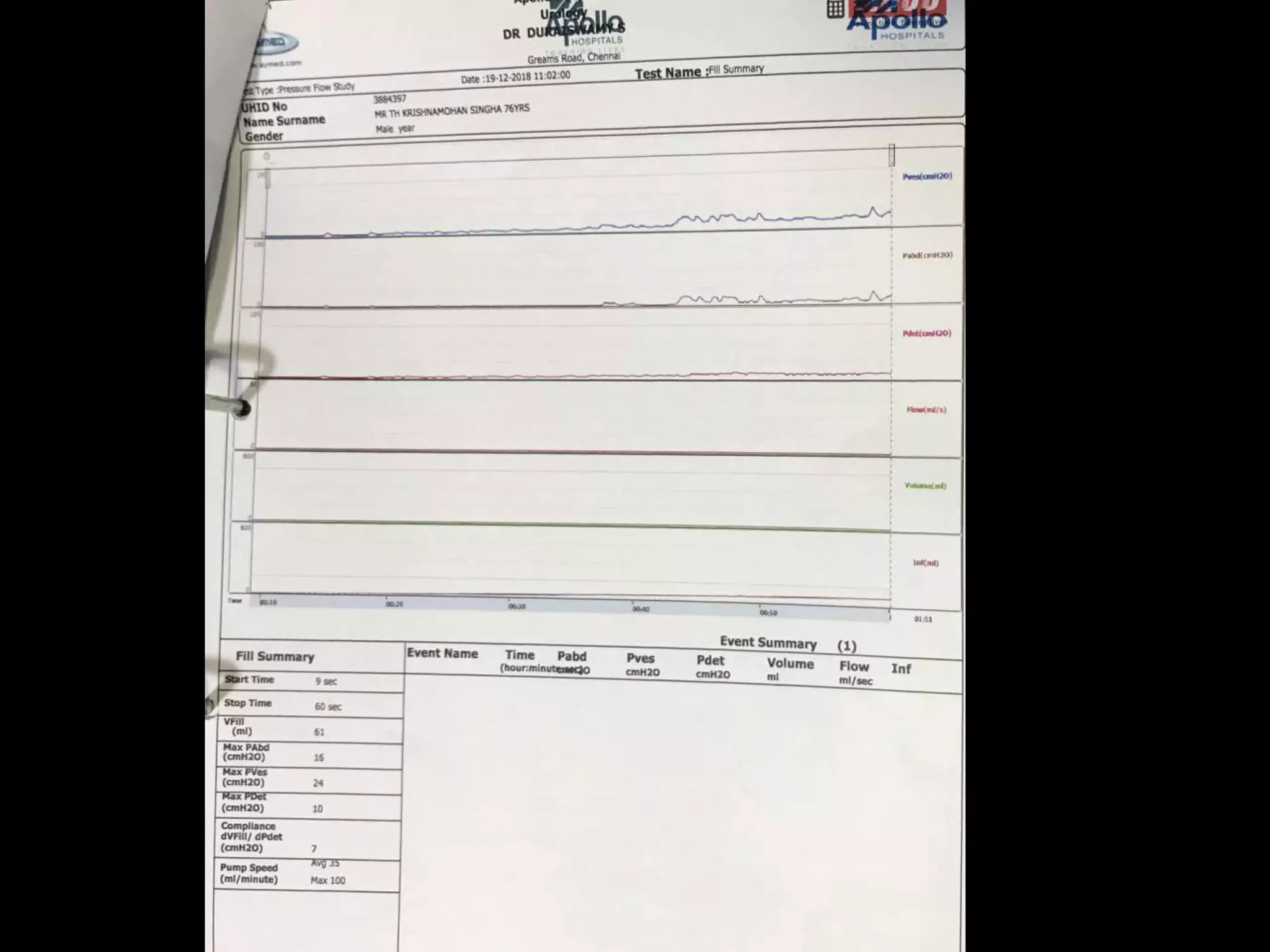

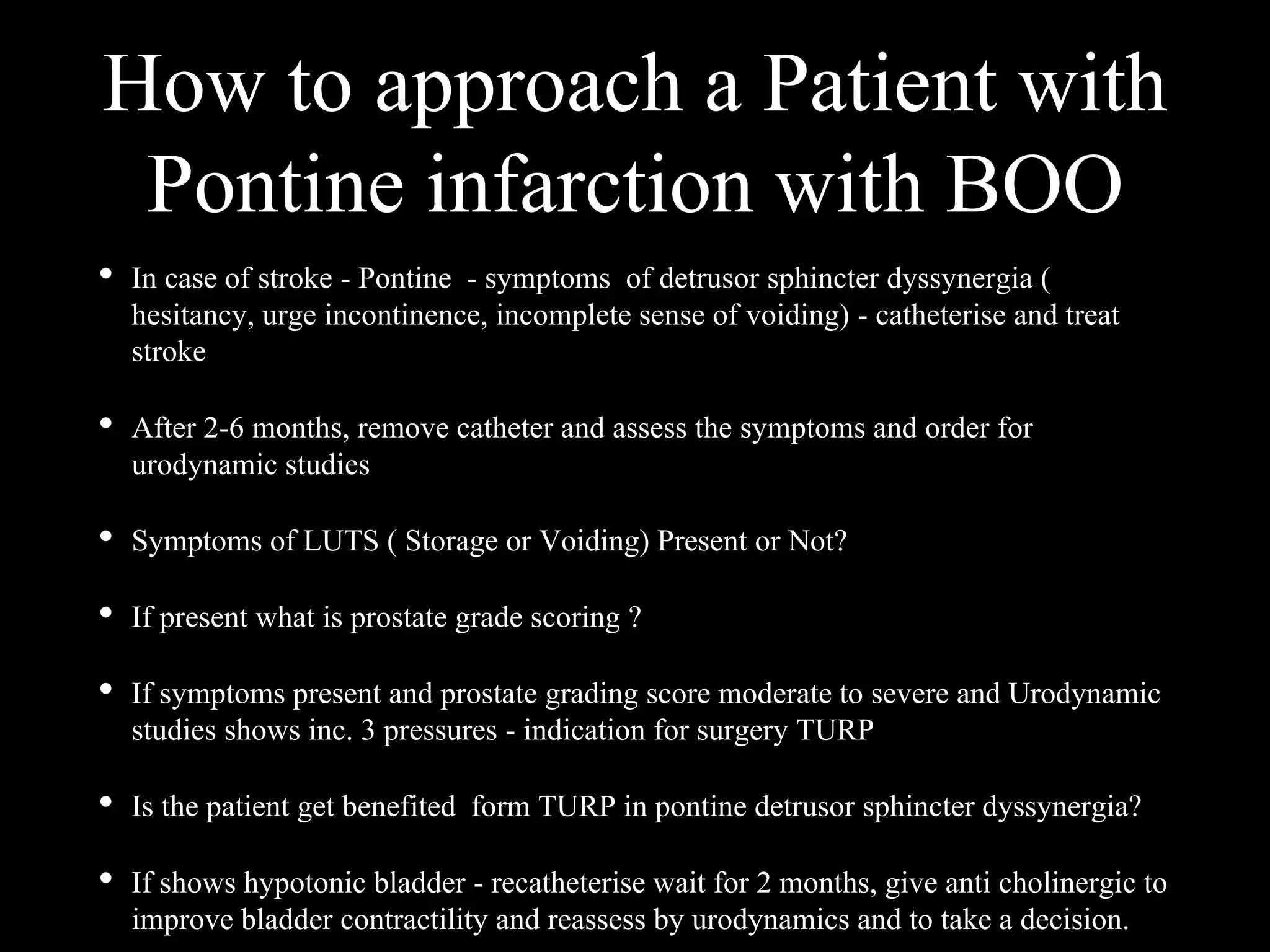














The document presents a case study of a 73-year-old man with a history of diabetes and hypertension who developed urinary incontinence following an acute stroke. He exhibits symptoms of detrusor sphincter dyssynergia and has been catheterized for management. The evaluation suggests a need for urodynamic studies and potential surgical intervention based on prostate grading and bladder functionality.




































![Incontinence & Female Urology [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/incontinencefemaleedmond-140716213134-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

















































