Downloaded 602 times



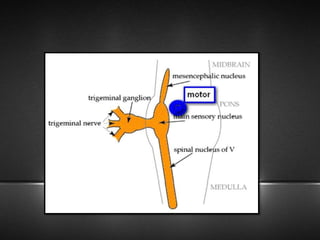

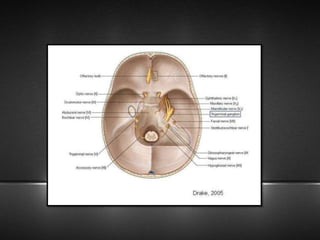

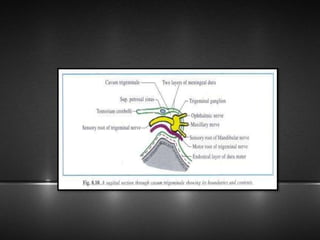
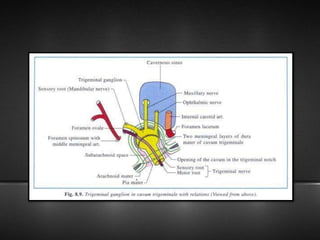
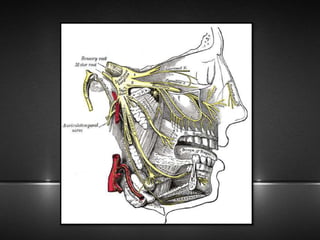
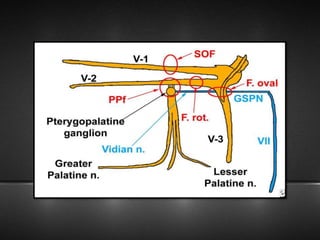
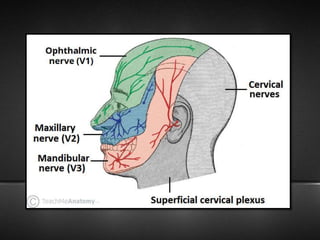
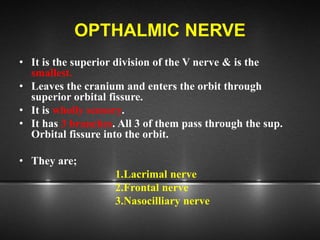
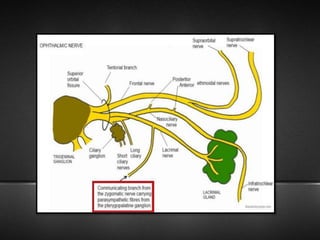
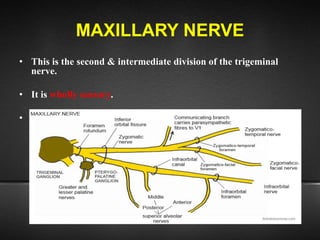
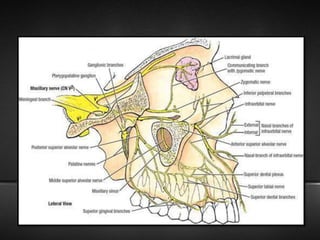
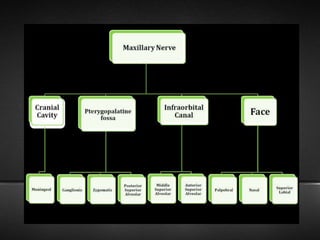

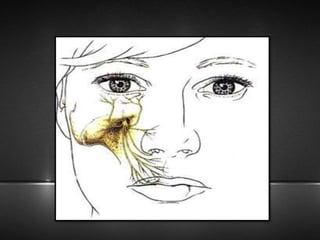

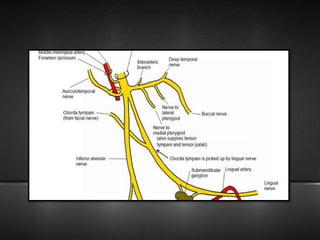
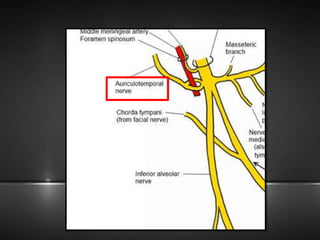
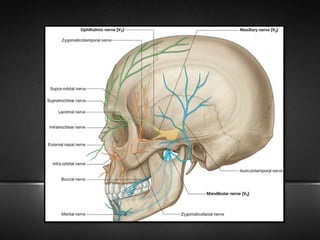

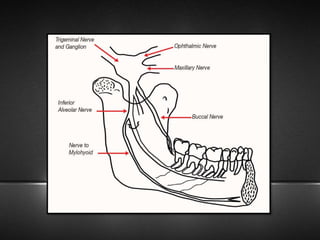
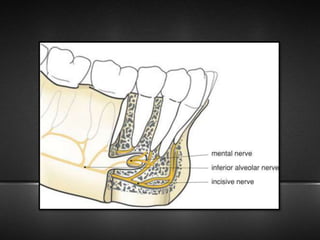

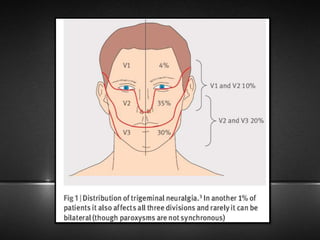




The document provides information about the trigeminal nerve (CN V), which is the largest of the cranial nerves. It has both sensory and motor components. The trigeminal nerve has three main divisions - the ophthalmic, maxillary, and mandibular nerves. It innervates most of the face and provides sensory innervation to the teeth and oral cavity. The trigeminal nerve nuclei are located in the pons and midbrain. The trigeminal ganglion contains the cell bodies of pseudounipolar neurons. The branches and distribution of the three divisions of the trigeminal nerve are described in detail.




























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






