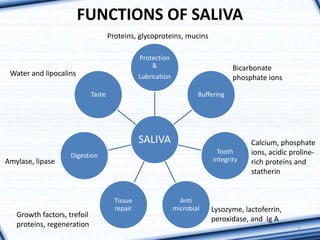
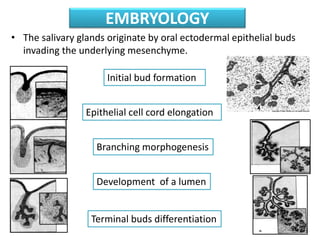
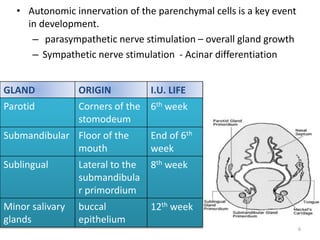
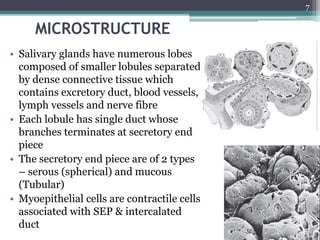
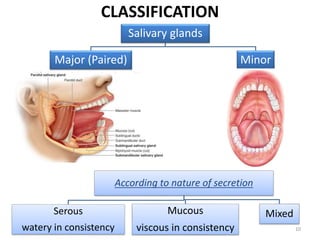
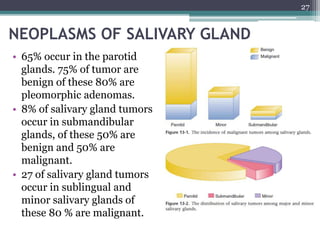
1. The document provides information on the salivary glands, including their embryology, microstructure, classification, and the surgical anatomy of the major salivary glands - the parotid and submandibular glands.
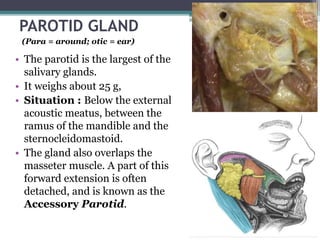
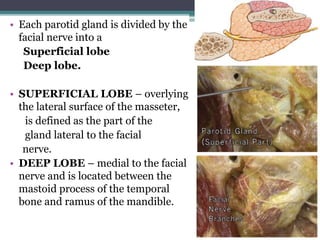
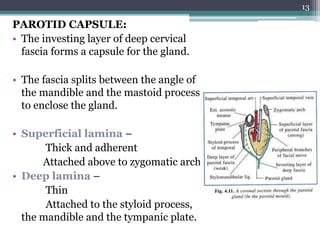
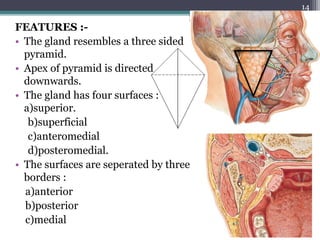
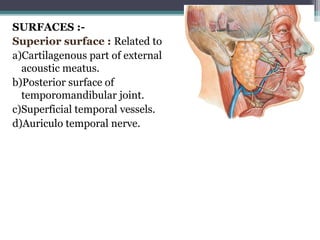
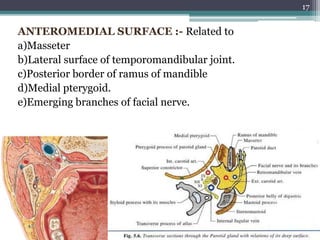
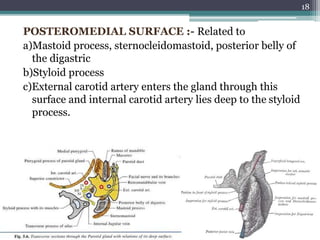
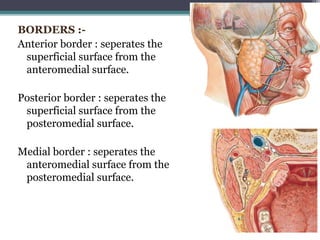
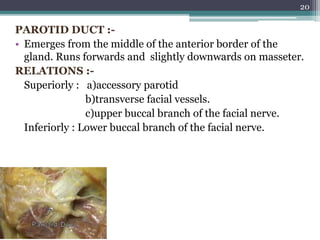
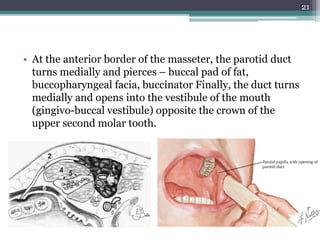
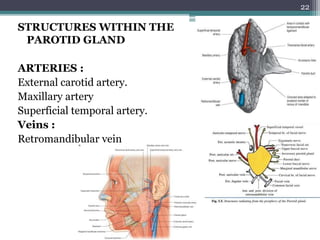
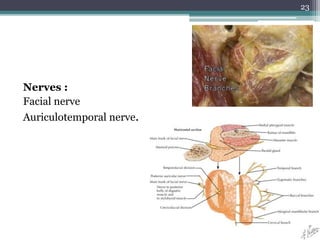
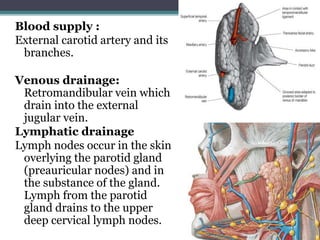
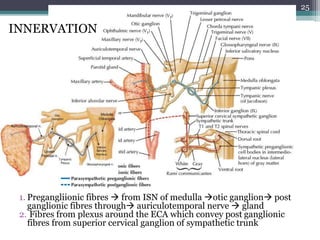
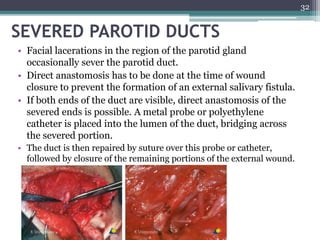
2. It describes the parotid gland as the largest salivary gland, located below the external ear. It discusses the gland's lobes, surfaces, borders, duct, blood supply and innervation.
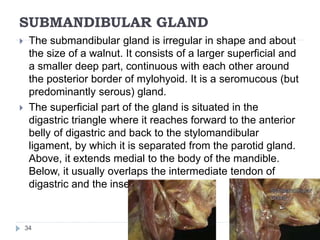
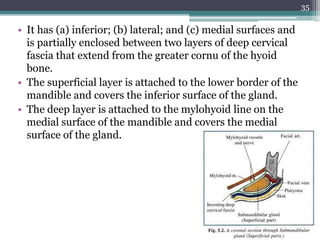
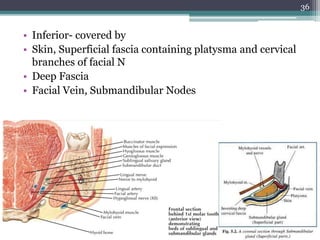
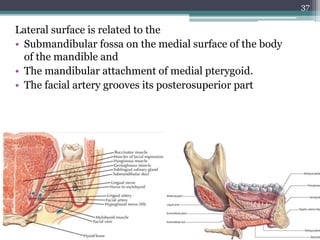
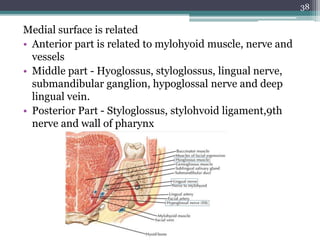
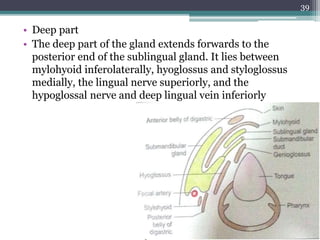
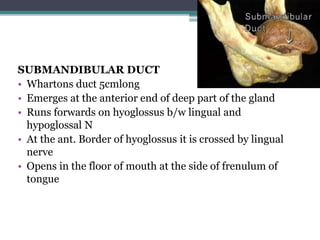
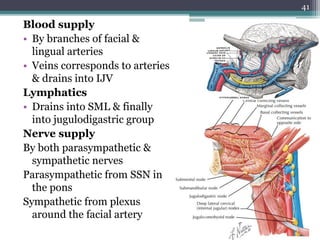
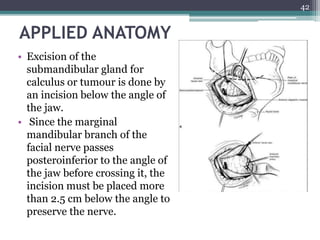
3. It also summarizes the submandibular gland, located in the submandibular triangle, discussing its parts, surfaces, duct, blood supply and innervation.