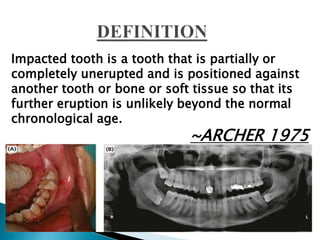
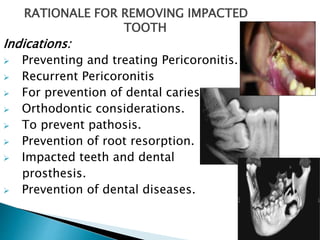
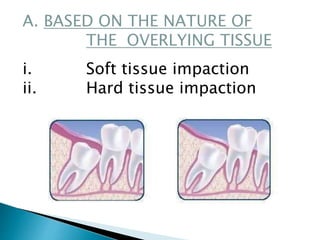
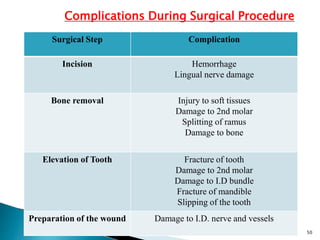
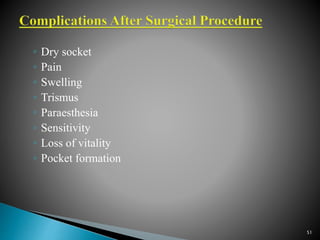
This document summarizes information about impacted teeth. It begins by defining an impacted tooth and listing the most common sites of impaction. It then discusses several theories for the causes of impaction, including lack of space from small jaws, heredity, pathology, endocrinology, and nature versus nurture. Risk factors and classifications of impacted teeth are also outlined. The document provides details on the rationale for removal, contraindications, surgical techniques, complications, and postoperative care for impacted teeth.