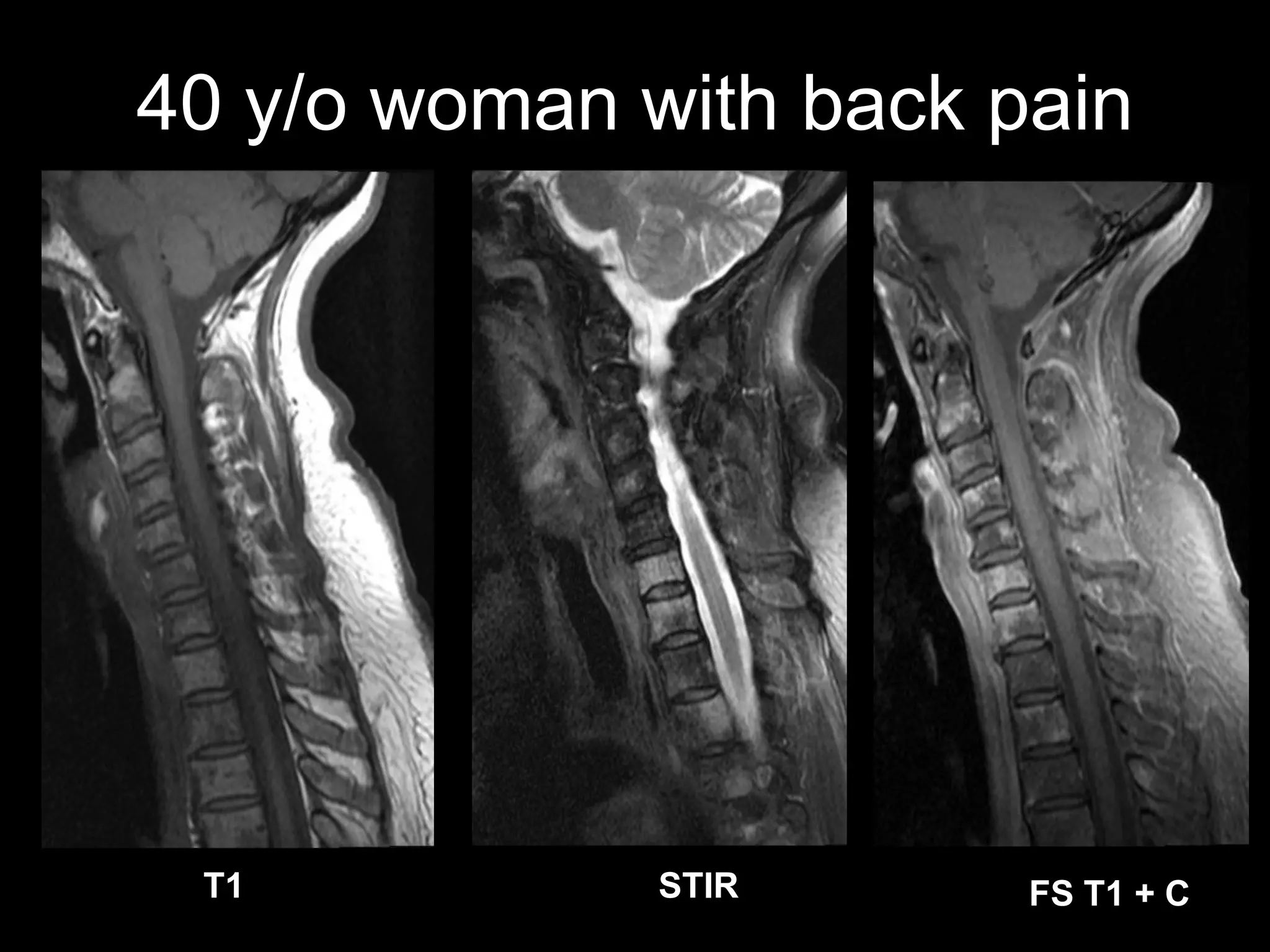
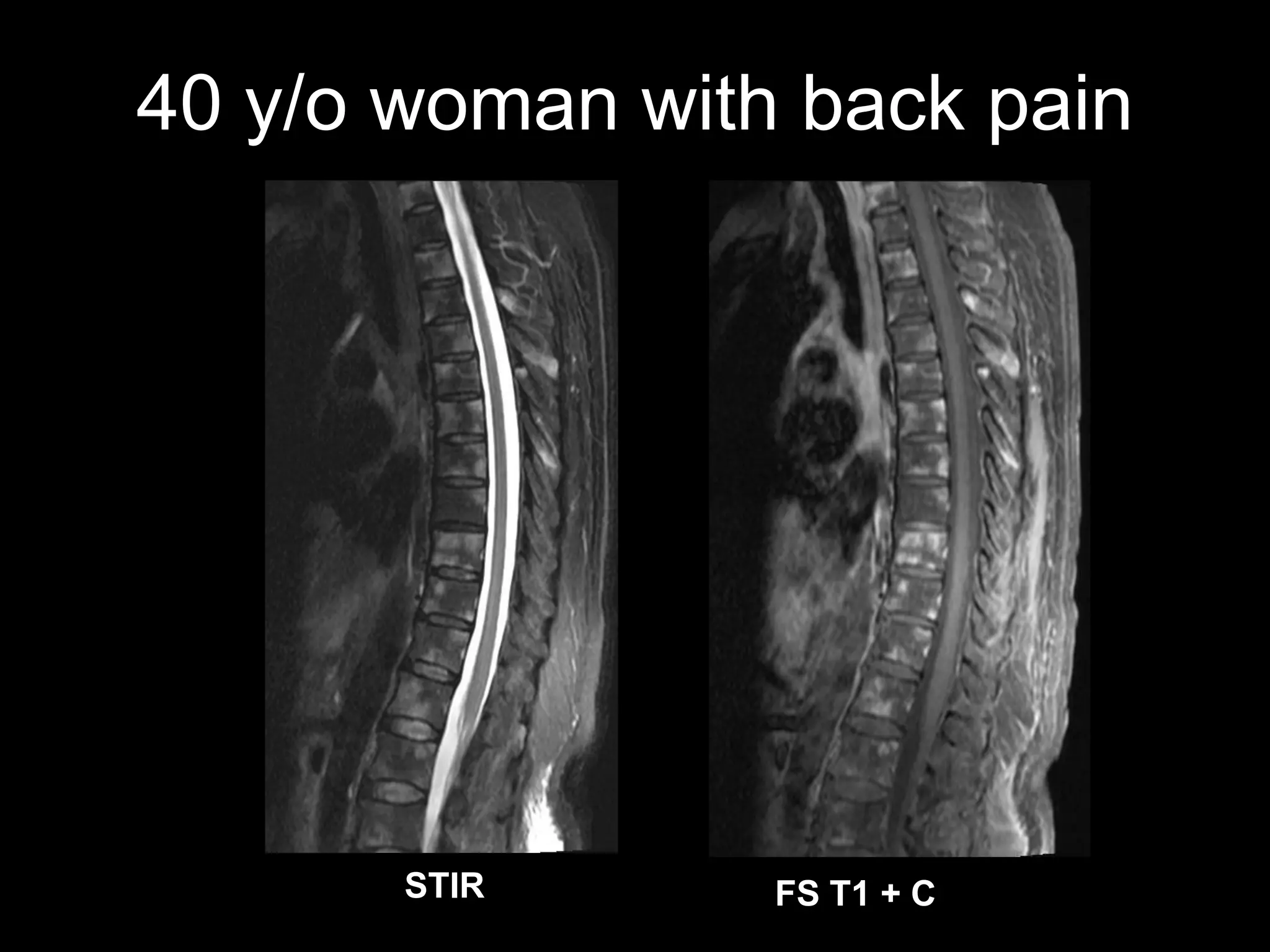
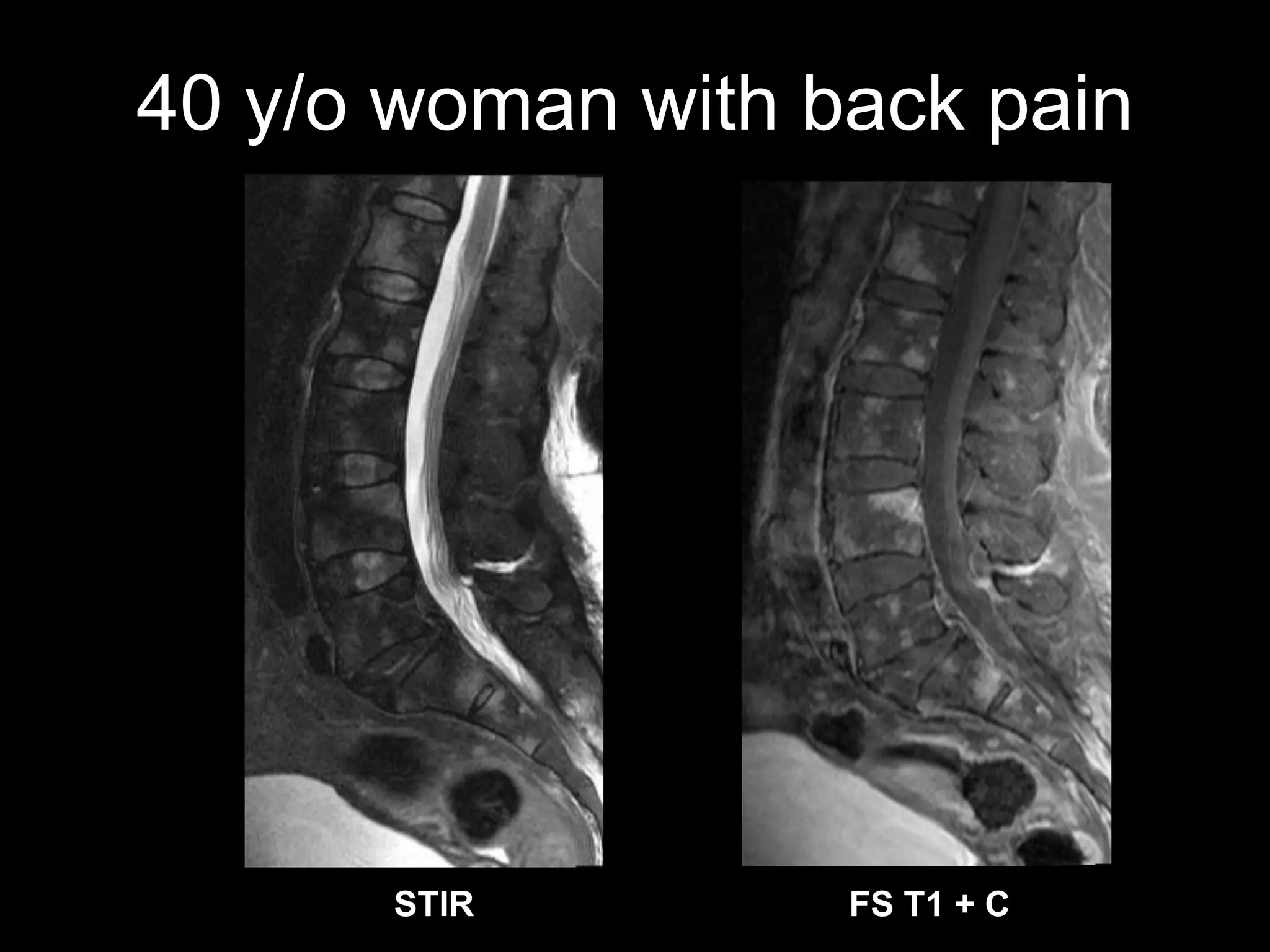
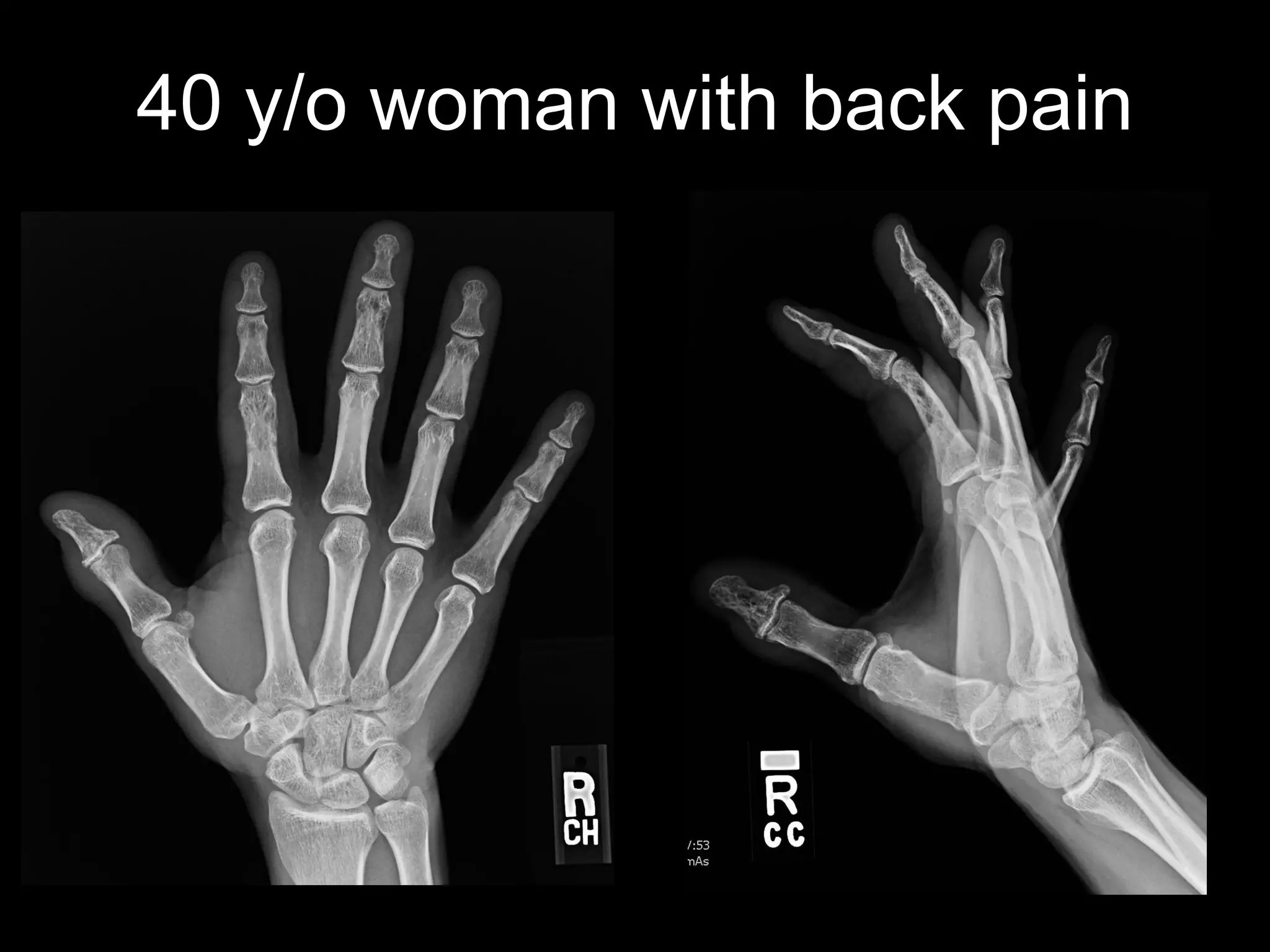
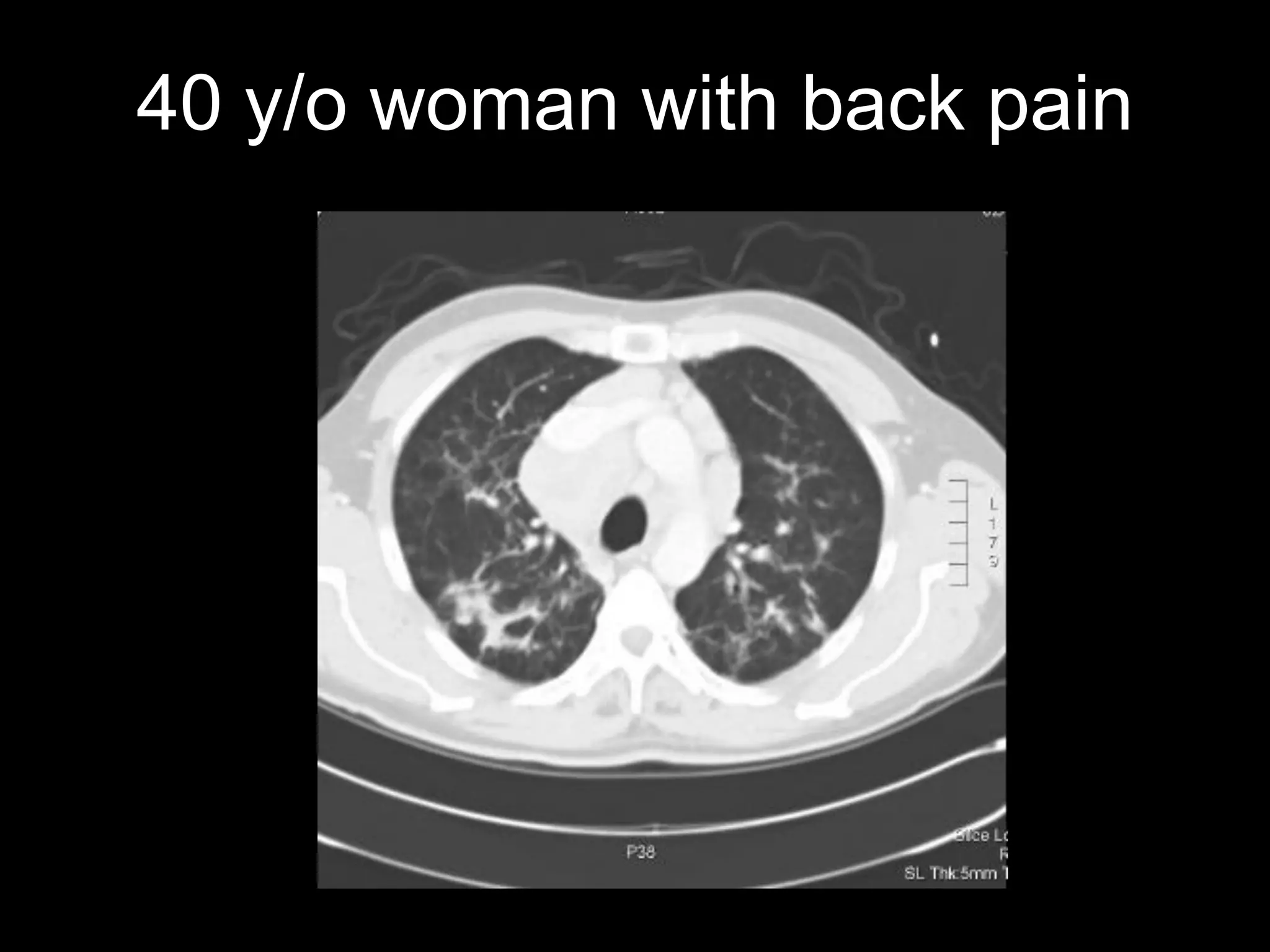
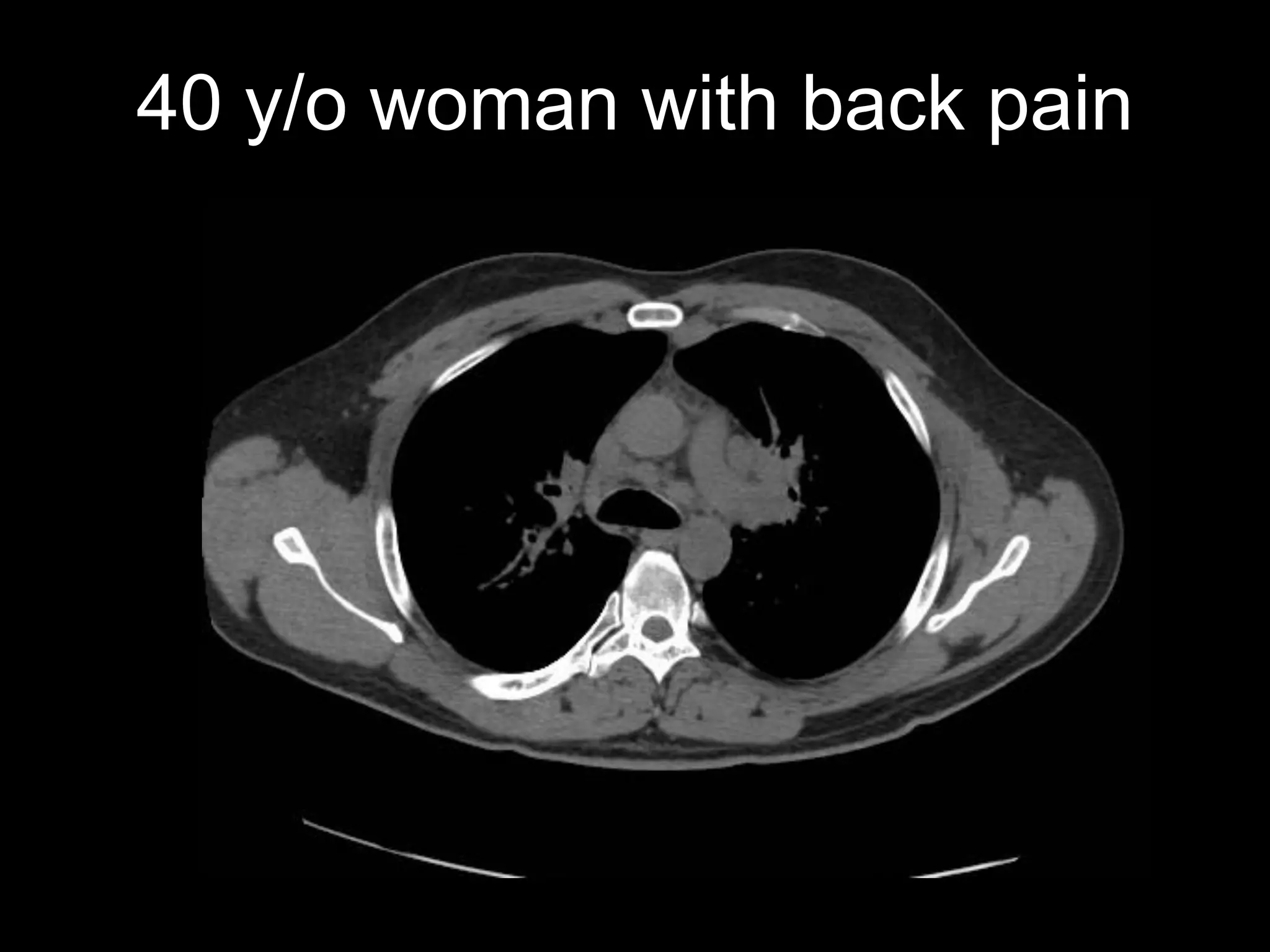
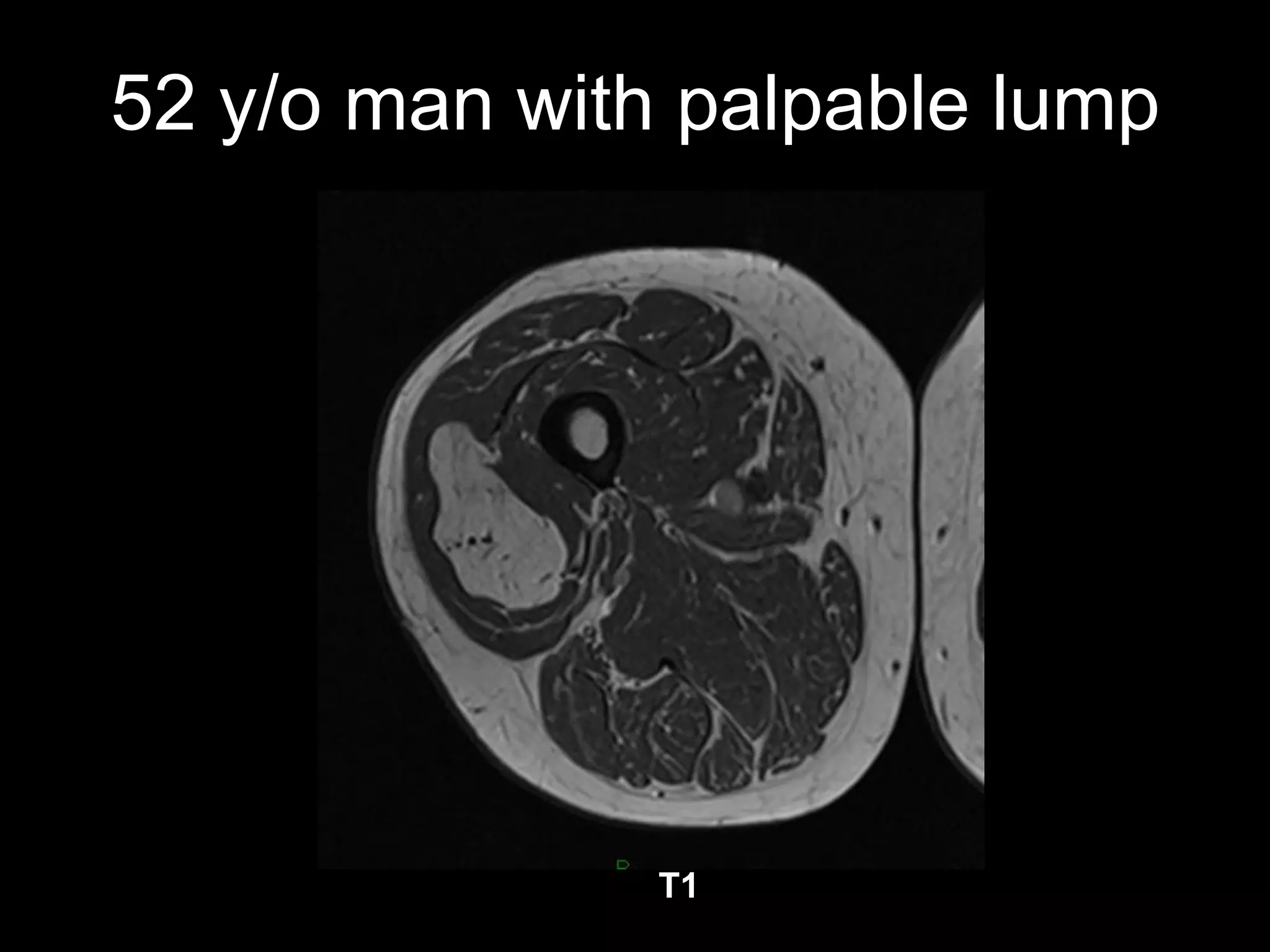
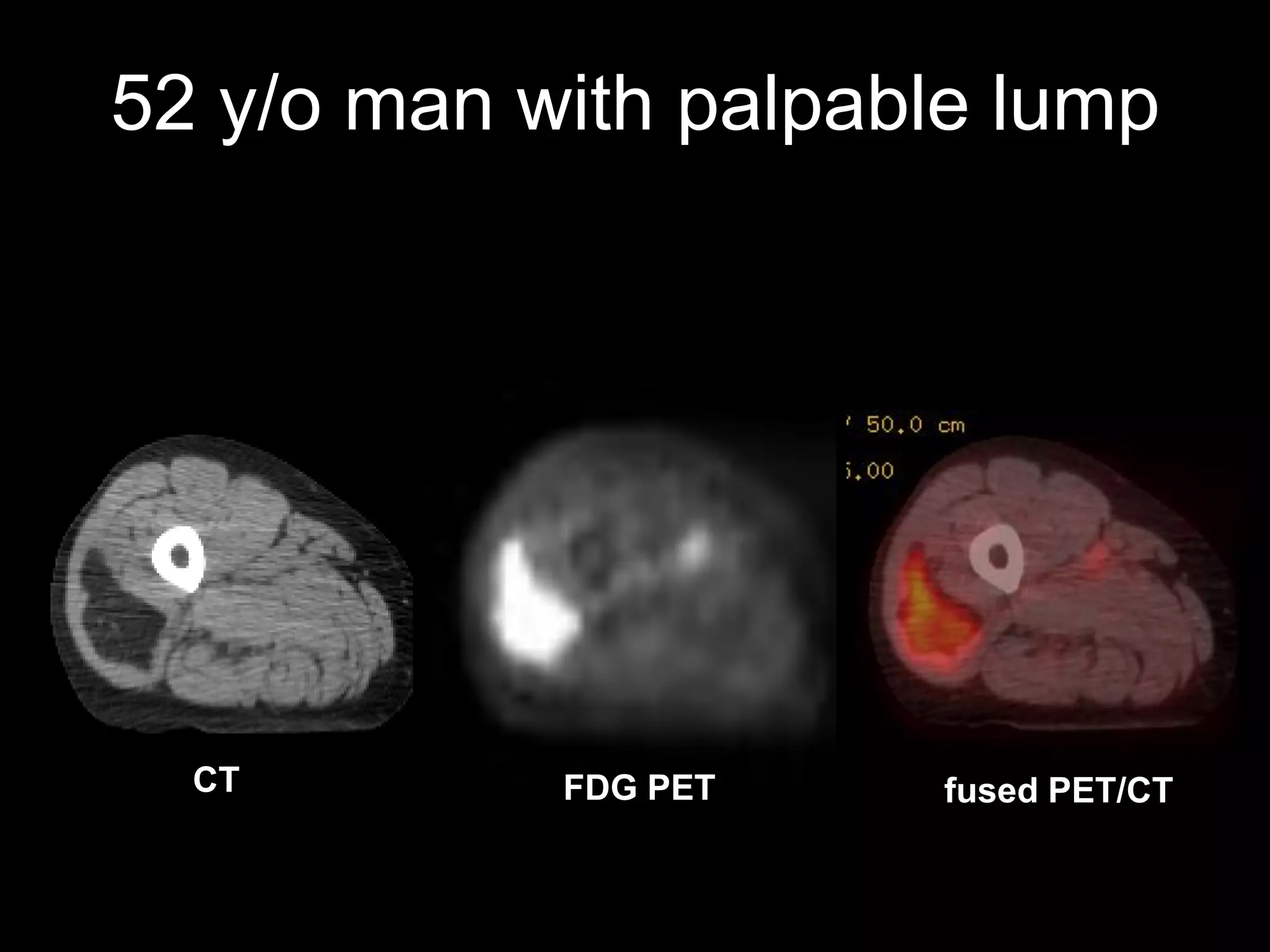
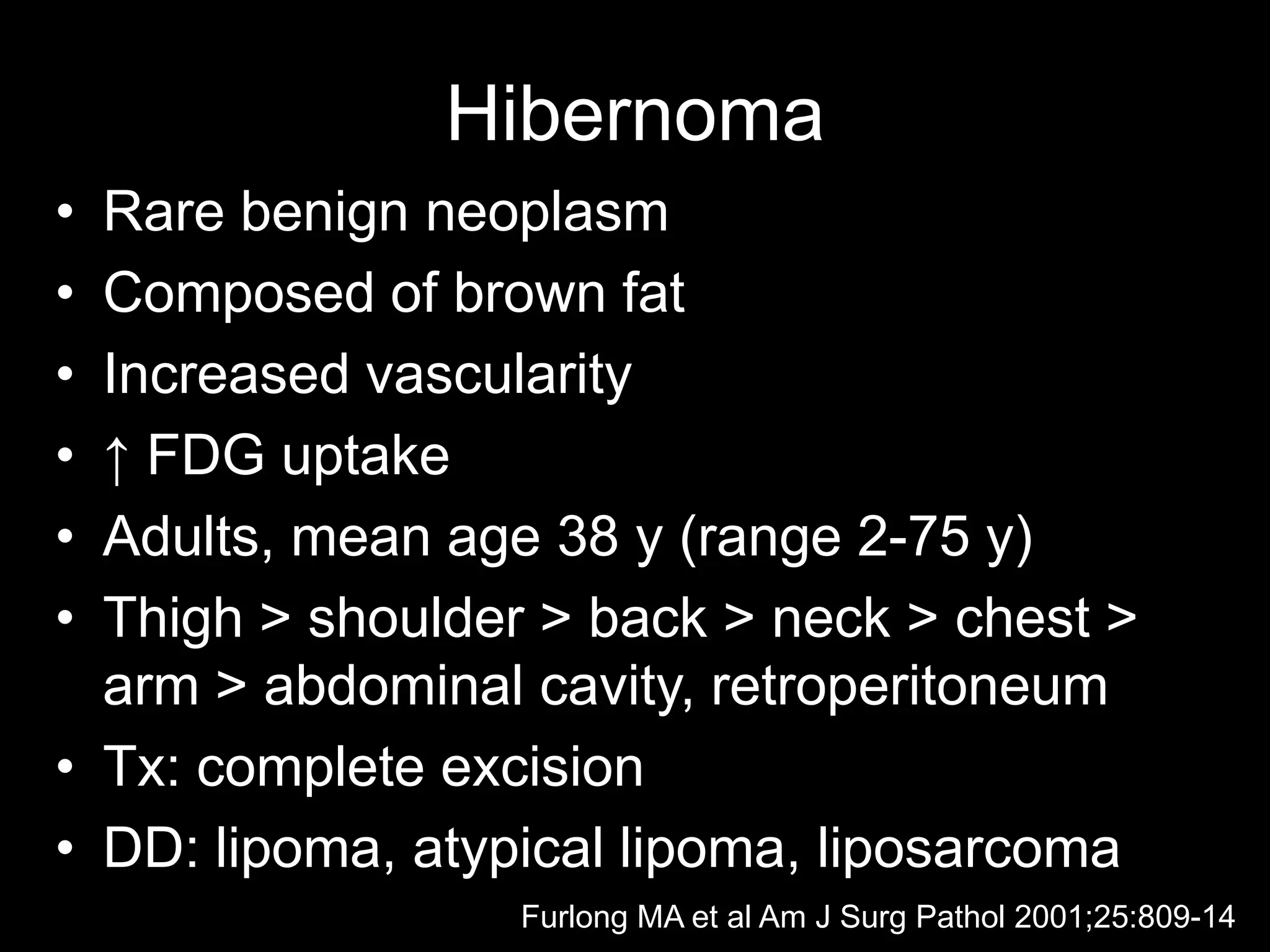
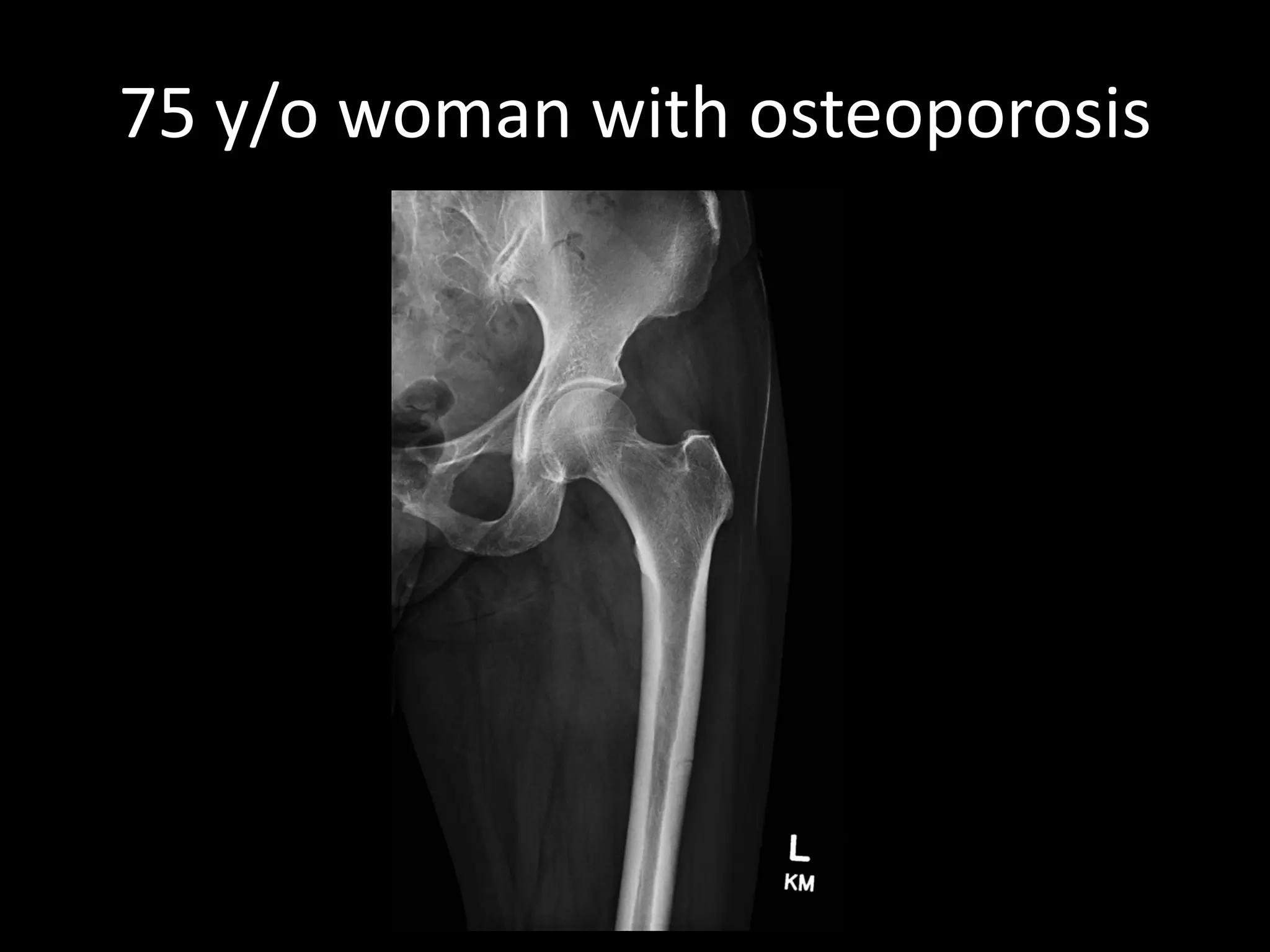
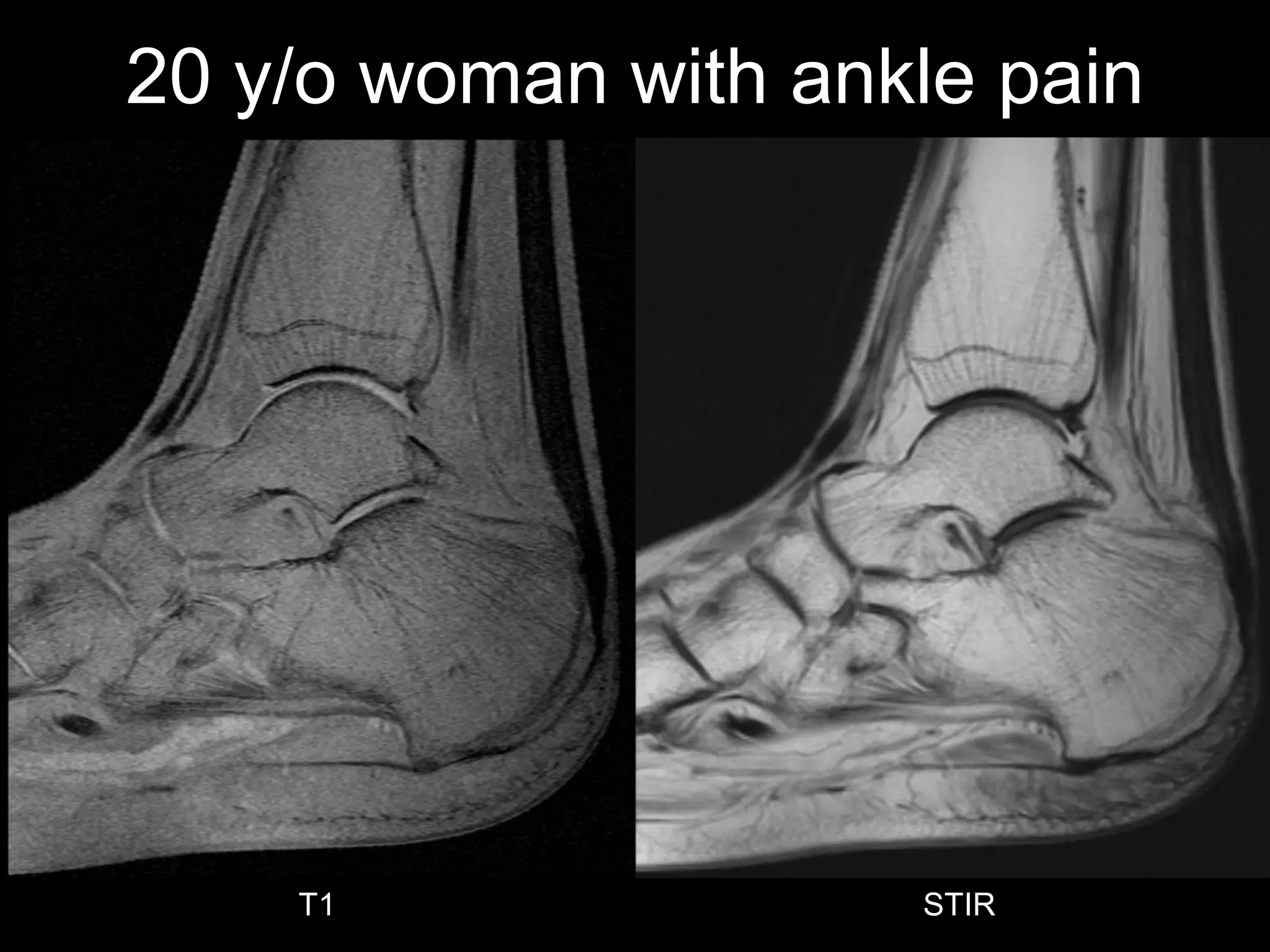
This document presents several unknown medical cases involving imaging findings. It discusses cases of a 40-year-old woman with back pain and possible sarcoidosis, a 52-year-old man with a palpable lump evaluated with CT and PET/CT showing a rare hibernoma tumor, and a 75-year-old woman with osteoporosis and an atypical femoral fracture potentially related to long-term bisphosphonate use. It also briefly summarizes a case of serous atrophy in a 20-year-old woman with ankle pain.











![Wilm's tumour - The most common kidney tumor in children - Dr Vishnu A [VCR],...](https://cdn.slidesharecdn.com/ss_thumbnails/vishnu-wilmstumour-210312145616-thumbnail.jpg?width=640&height=640&fit=bounds)

















































































