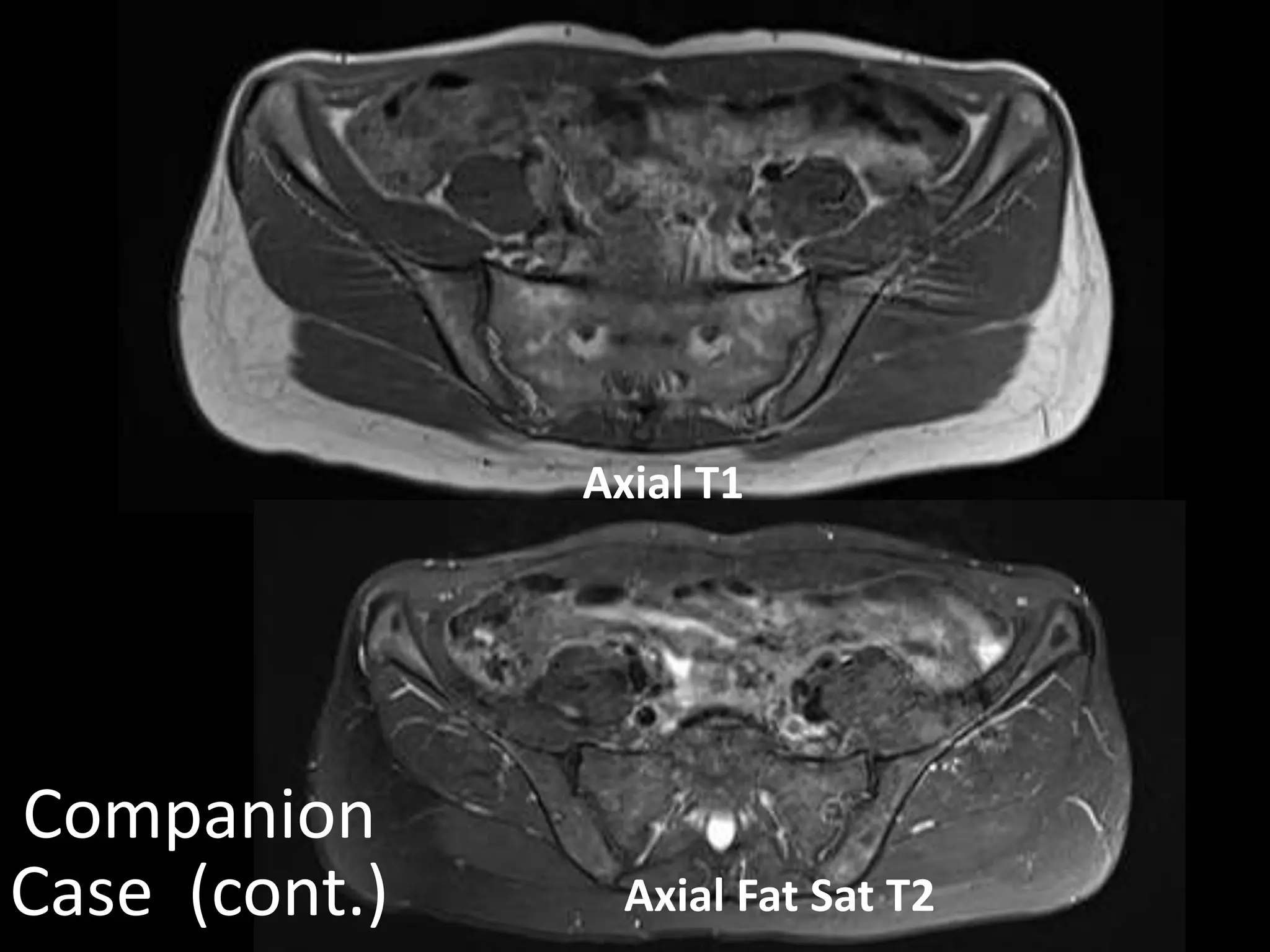
Case 1 - A 40-year-old woman with a history of lymphoma in remission presents with left hip pain. Imaging shows abnormalities at the left anterior iliac crest. A companion case involves a 43-year-old woman with pain at the right anterior iliac crest.
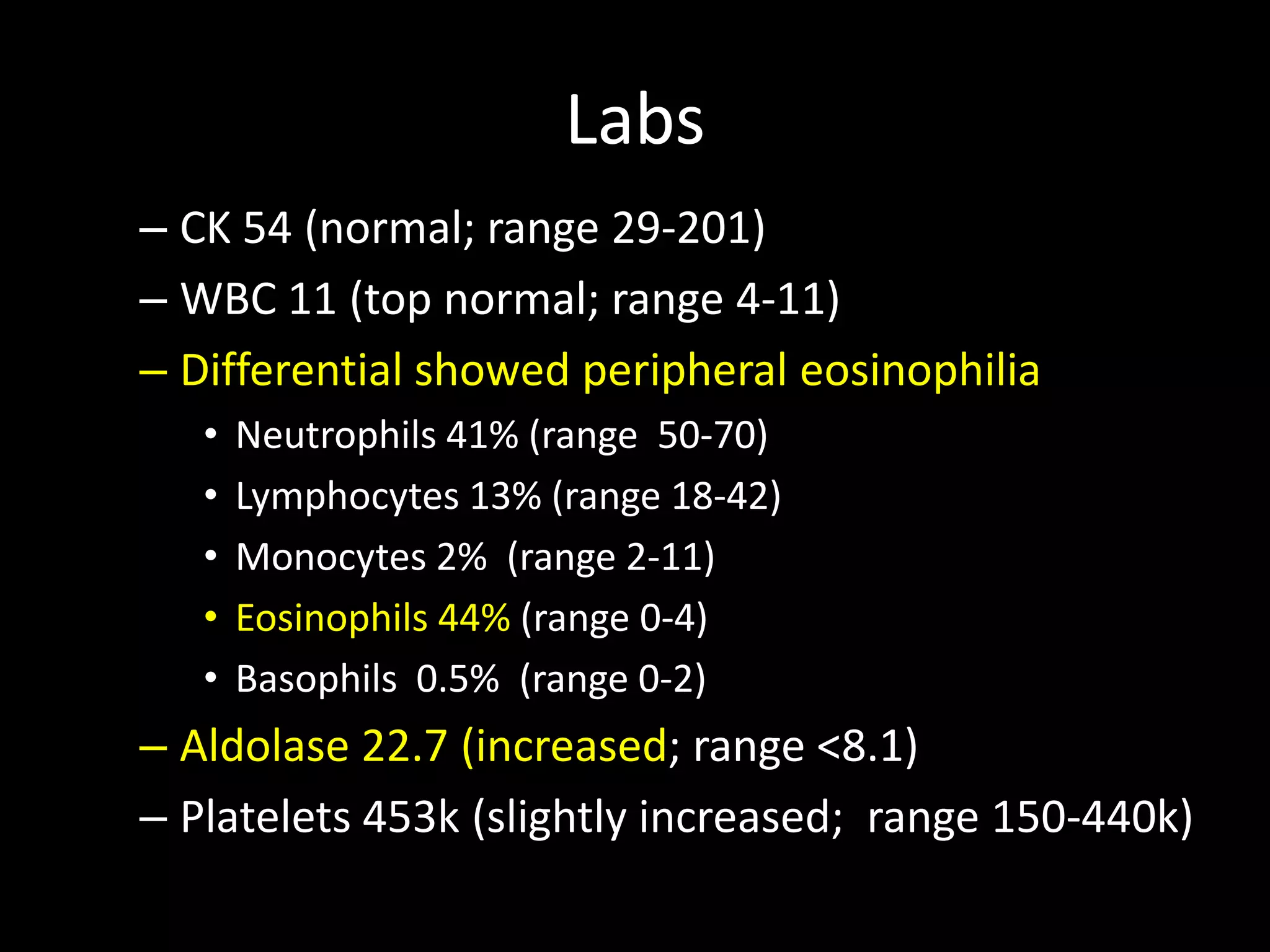
Case 2 - A 27-year-old runner developed weakness and edema over 4 months. Labs show peripheral eosinophilia. MRI shows abnormalities of the thighs.
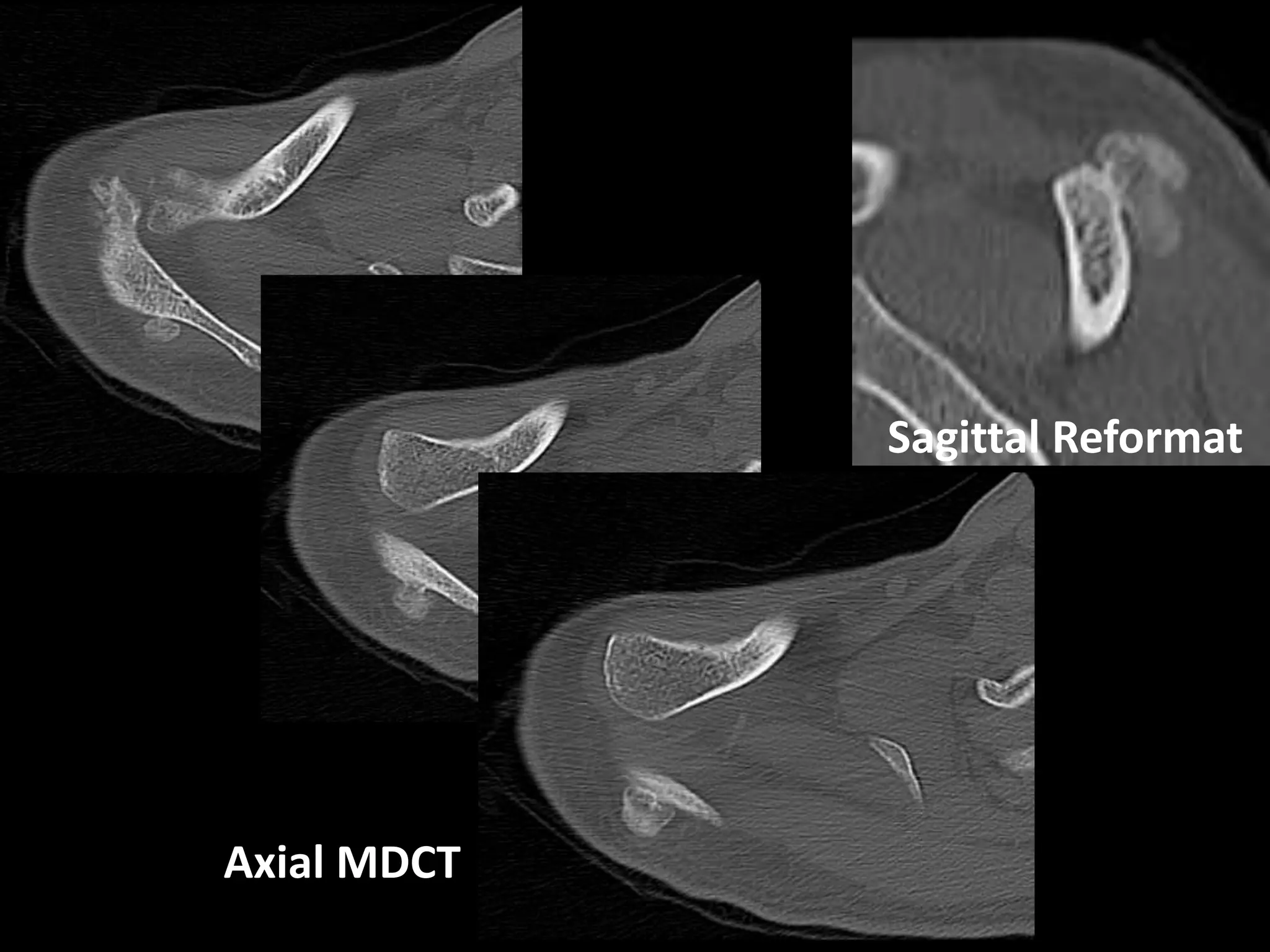
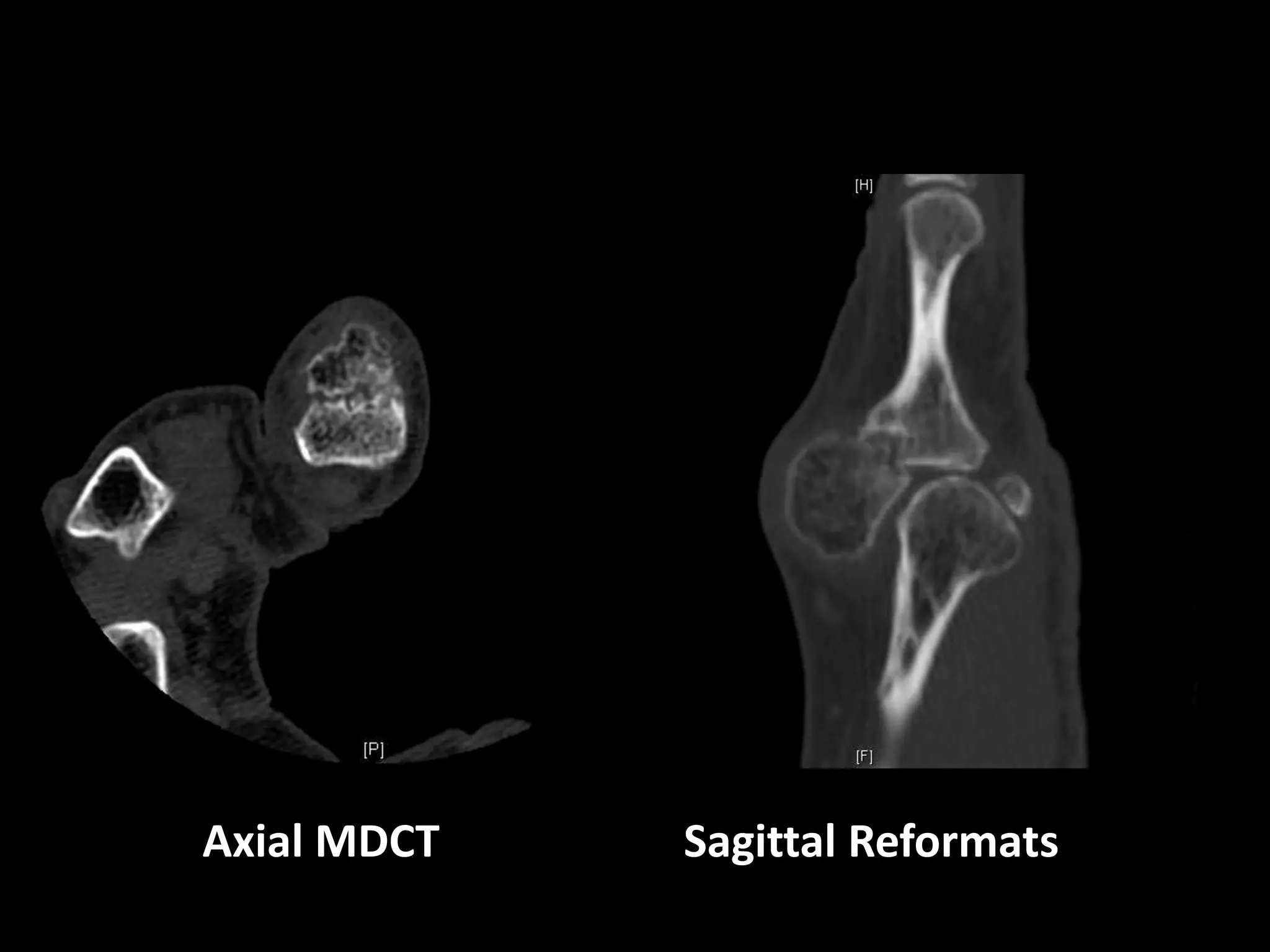
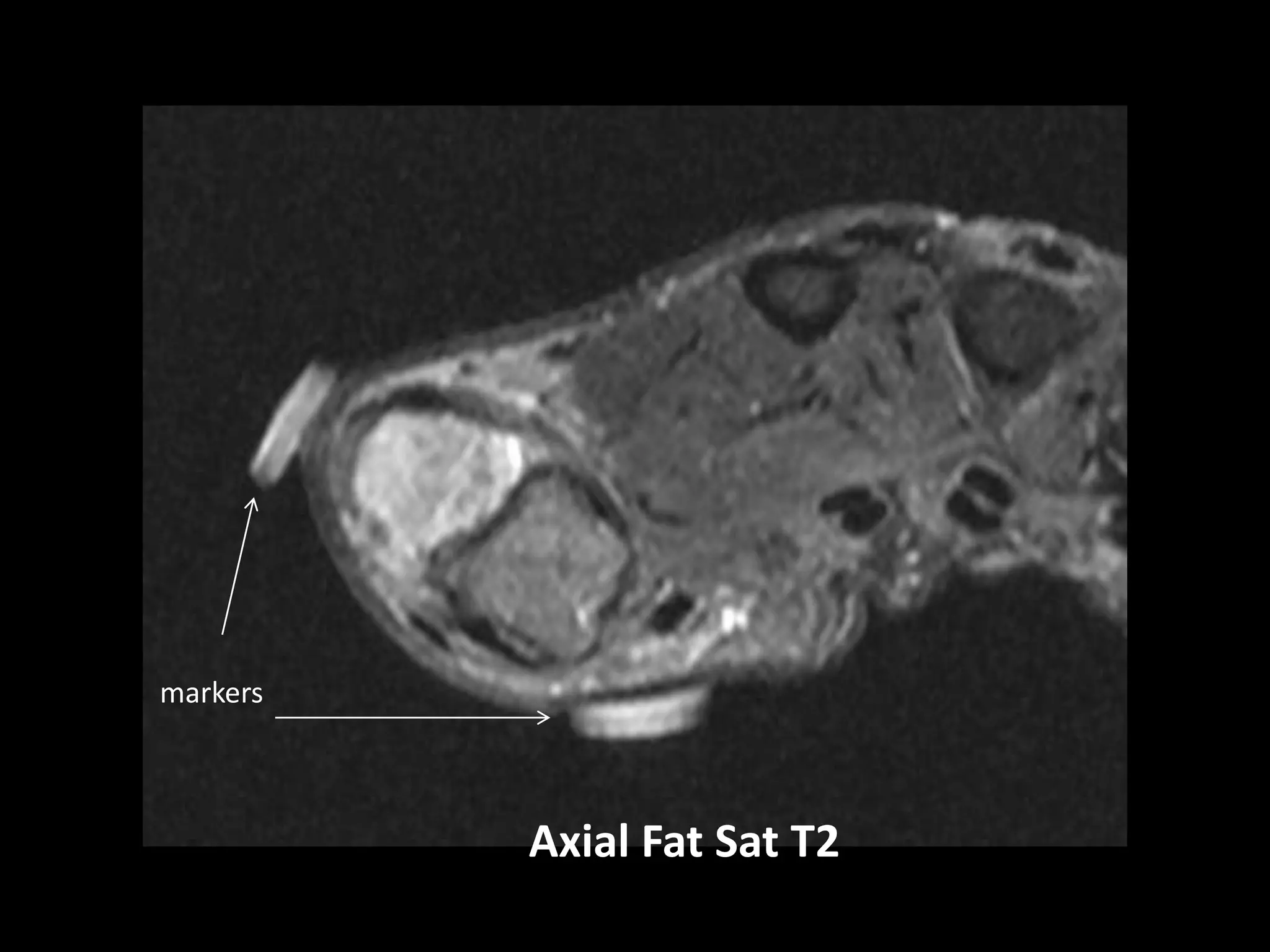
Case 3 - A 32-year-old man noted a firm right shoulder mass. Imaging shows a scapular mass and a companion case of a more common presentation of the same entity in the thumb.
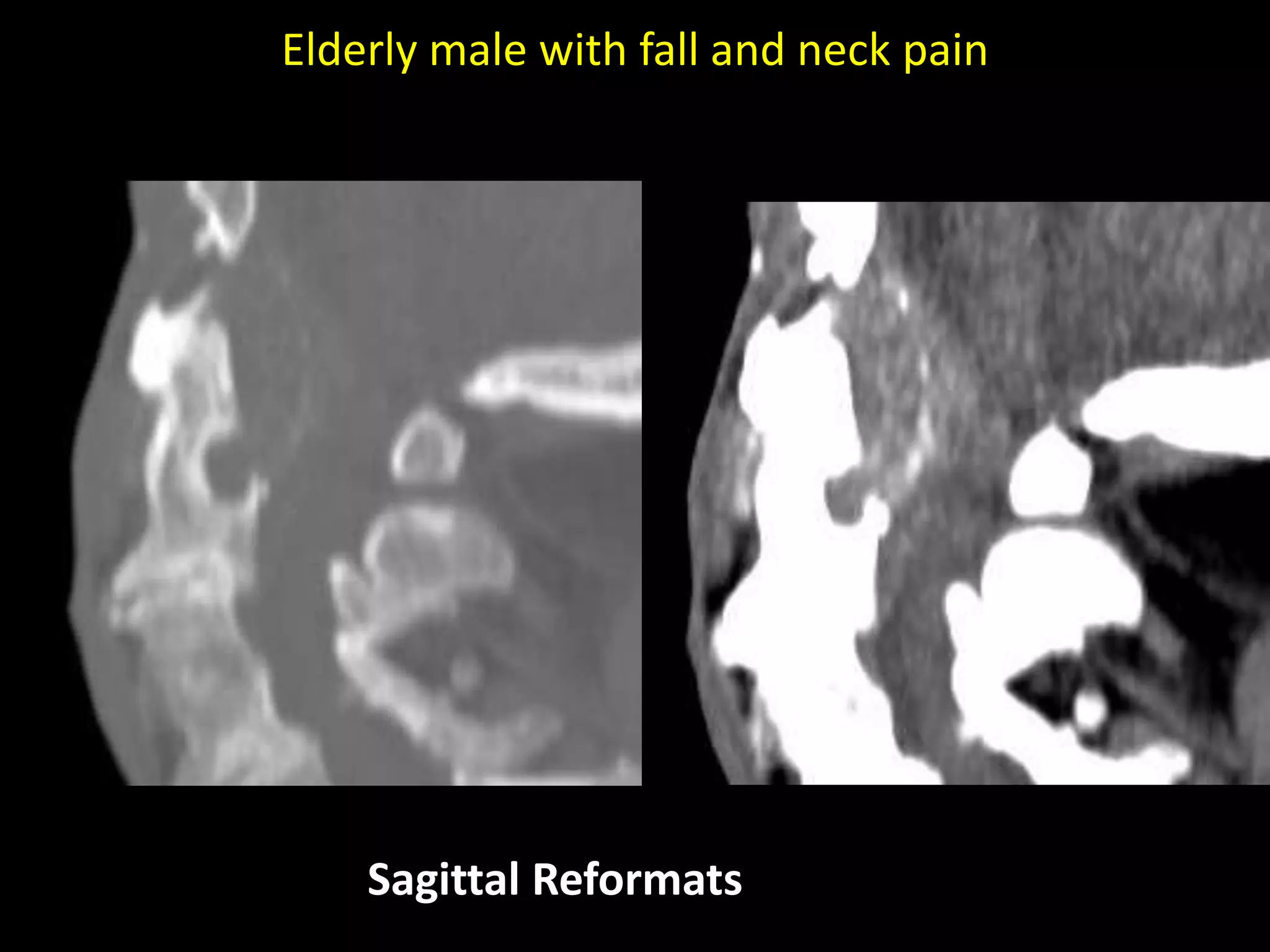
Case 4 - An 84-year-old man