The document discusses various primary retroperitoneal neoplasms. It describes the location of the retroperitoneum and divides primary retroperitoneal neoplasms into solid neoplastic masses including mesodermal neoplasms (such as liposarcomas, leiomyosarcomas, and malignant fibrous histiocytomas), neurogenic tumors, and germ cell/sex cord/stromal tumors. For each type of neoplasm, it provides details on characteristics such as common subtypes, demographic and imaging appearances, and clinical implications.























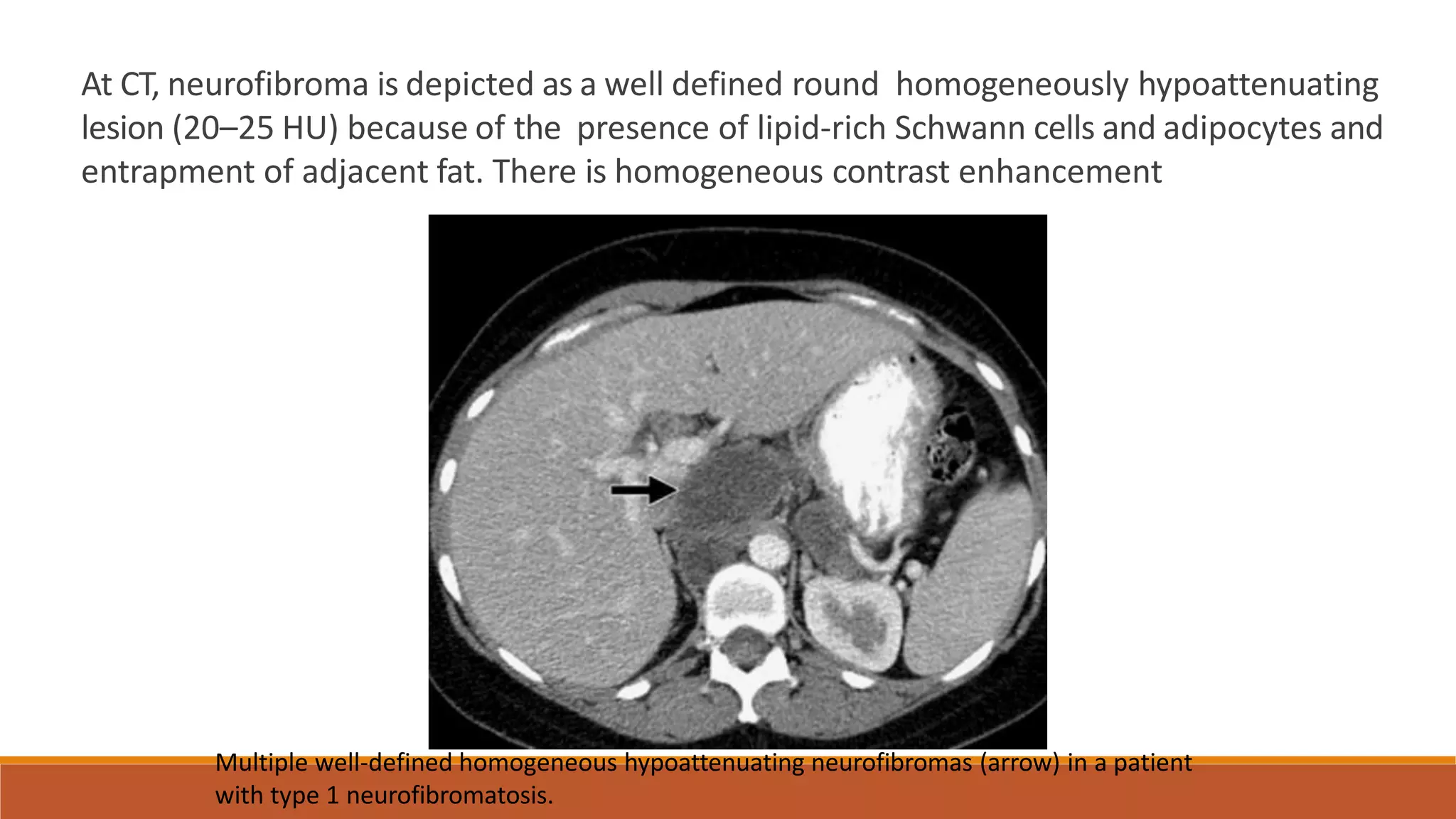
![NEUROGENIC TUMORS
Neurogenic tumors constitute 10%–20% of primary retroperitoneal
tumors.
Compared with the mesenchymal tumors, neurogenic tumors occur in a
younger age group and are more likely to be benign and have a better
prognosis.
Neurogenic tumors can originate from the
1. nerve sheath (schwannoma, neurofibroma, neurofibromatosis,
malignant nerve sheath tumors [malignant schwannoma,
Neurofibrosarcoma]),
2. ganglionic cells (ganglioneuroma, ganglioneuroblastoma,
neuroblastoma)
3. paraganglionic cells (paraganglioma, pheochromocytoma).](https://image.slidesharecdn.com/retroperitonealmasses-230430182519-11a71d19/75/retroperitoneal-masses-pptx-25-2048.jpg)